Chapter III. The Thorax
Description
This section is from the book "Landmarks And Surface Markings Of The Human Body", by Louis Bathe Rawling. Also available from Amazon: Landmarks and Surface Markings of the Human Body.
Chapter III. The Thorax
The majority of the thoracic viscera are depicted on the surface in relation to the costal cartilages, ribs and intercostal spaces, and it is therefore necessary to lay stress on certain important points :
1. That the twelve ribs are divided into two groups: (a) True ribs, seven in number, articulating by means of their costal cartilages with the mesial sterno-xiphoid bone ; (b) False ribs, five in number, all falling short of the middle line, the upper three attached to the costal cartilage of the rib above, the lower two not articulating with the transverse process of the corresponding vertebra, and the anterior extremities not attached to the costal cartilage of the rib above. These last two ribs are therefore known as " floating ribs."
2. That the first rib lies mainly under cover of the clavicle, but that its costal cartilage can generally palpated with ease as it lies below the sternal end of the clavicle. (Fig. III, 23.)
3. That the first interspace which can be felt to the outer side of the sternum is the first interspace. This axiom may appear at first sight to be quite unnecessary, but it is in reality not uncommon for students to regard the first space which can be felt as the second interspace.
4. That the second costal cartilage articulates in front at the angle of Ludwig with the adjoining parts of the manubrium and gladiolus. (Fig. III, 20, 22)
5. That the seventh costal cartilage articulates with the adjoining parts of the gladiolus and xiphoid cartilage. Fig. XVII.
6. That the anterior extremity of the ninth costal cartilage corresponds almost exactly to the point where the linea semilunaris cuts the costal arch. Fig. XX.
7. That the twelfth rib is liable to great variation in size, frequently being so insignificant that it cannot be felt at all. It is, therefore, often advisable to count from above in fixing any particular rib.
8. That the intercostal spaces, in consequence of the downward and forward obliquity of the ribs, are wider in front than behind.
The female mamma, when well developed, extends upwards to the second rib, inwards to the outer border of the sternum, downwards to the sixth or seventh rib, and outwards to the mid-axillary line. The true glandular substance is, however, less regular in disposition, prolongations passing in various directions. Of these, the most important is the so-called " axillary prolongation," which is directed upwards and outwards along the anterior fold of the axilla.
The nipple usually corresponds to the fourth interspace It is variable in position, and not infrequently overlies the fourth rib. In the female the nipple lies just below, and external to, the apex or central point of the breast. Fig. XV.
The heart lies opposite the middle four dorsal vertebra, Fig. XV, 1-4. and the projection of its anterior surface upon the front of the chest wall may be indicated in the following manner.
Take the following four points :
1. The lower border of the second left costal cartilage about 1 inch from the left border of the sternum.
2. The upper border of the third right costal cartilage 1/4 to 1/2 inch from the right border of the sternum.
3. The lower border of the sixth right costal cartilage 3/4 inch from the right border of the sternum.
4. The fifth left interspace 1 1/2 inches below and just internal to a line drawn vertically downwards from the nipple. If any abnormality exists with regard to the position of the nipple, this last point may be fixed with greater accuracy by taking a point in the fifth left interspace nearly 4 inches from the middle line.
The apex beatthe point of maximum impulse of the left ventricle against the chest wall (Fig. XV, 8.) lies in the fifth left interspace 1 1/2 inches below and 1/2 inch internal to the nipple, or 3 1/2 inches from the middle line. The position of the apex beat, therefore, does not exactly represent the outermost limit of the left ventricle. The above four points should now be joined in the following manner :
Points 1 and 2 by a straight line.
Points 2 and 3 by a curved line, the heart reaching the greatest distance from the middle line, 1 1/2 inches, in the fourth interspace.
Points 3 and 4 by a line presenting a slight downward convexity, and cutting across the middle line in close relation to the xiphisternal junction.
Points 1 and 4 by a line presenting a fairly well marked convexity to the left. In the illustration this line is drawn rather too straight.
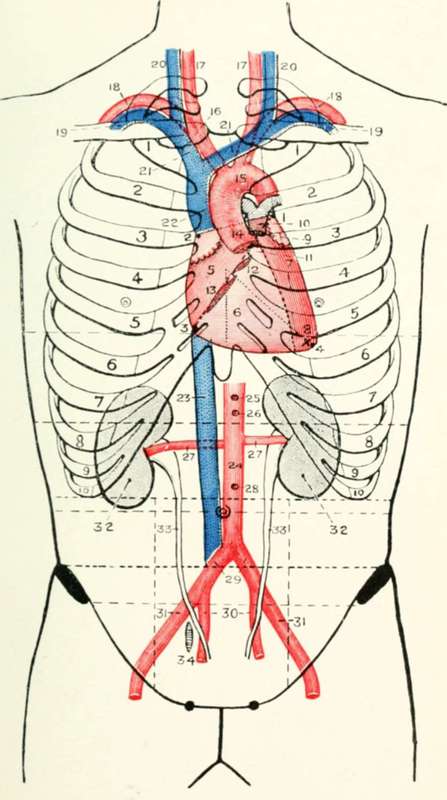
Fig. XV. The Heart, Great Vessels, Kidney, And Ureter
1-4. The four points of the heart.
5. The auricular area.
6. The ventricular area.
7. The left ventricle.
8. The apex beat.
9. The pulmonary valve.
10. The pulmonary artery.
11. The aortic valve.
12. The mitral valve.
13. The tricuspid valve.
14. The ascending aorta.
15. The aortic arch.
16. The innominate artery.
17. The right and left common carotid arteries.
18. The right and left subclavian arteries.
19. The right and left subclavian veins.
20. The right and left internal jugular veins.
21. The right and left innominate veins.
22. The superior vena cava.
23. The inferior vena cava.
24. The abdominal aorta.
25. The coeliac axis.
26. The superior mesenteric artery.
27. The renal arteries.
28. The inferior mesenteric artery.
29. The common iliac arteries.
30. The internal iliac arteries.
31. The external iliac arteries.
32. The kidney. 33. The ureters. 34. The ovary.
N.B
In this and in other figures in which the costal cartilages are depicted the numbered references do not refer to the corresponding cartilages. These are numbered for general convenience only.
A line joining Points 1 and 3 divides this cardiac area into two parts, (Fig. XV, 5.) which roughly correspond to the auricular area above and to the right, and the ventricular area below and to the left. This ventricular area is occupied mainly by the right ventricle, (Fig. XV, 6.) whilst a narrow strip along the left border represents that part of the left ventricle which comes to the surface. (Fig. XV, 7.)
The four points given above for marking out the projection of the heart on the anterior thoracic wall may be simplified by taking and joining the following four points :
1. The upper border of the third right chondro-sternal junction.
2. The lower border of the second left chondro-sternal junction.
3. The lower border of the sixth right chondro-sternal junction.
4. The position of the apex beat.
By uniting these four points, the heart is mapped out for most practical purposes with sufficient accuracy.
Continue to: