Chapter II. The Upper Extremity
Description
This section is from the book "Landmarks And Surface Markings Of The Human Body", by Louis Bathe Rawling. Also available from Amazon: Landmarks and Surface Markings of the Human Body.
Chapter II. The Upper Extremity
In this chapter, and in that on the lower extremity, the reader's attention is mainly directed to those bony prominences and muscular or tendinous elevations which lie in the region of the joints, since these form the more important landmarks which aid in the representation of the arteries, nerves, etc., of the limbs. The muscular masses, which complete the symmetry of the arm or leg between the joints, are only mentioned where necessary, a fair general knowledge of the anatomical structure of the body being assumed.
The Shoulder Region
The acromial process, the spine of the scapula and the clavicle, being subcutaneous throughout their whole length, can readily be palpated from end to end. The clavicle should first be examined from its blunted sternal extremity to the acromio-clavicular joint. The inner third of the shaft is rounded and presents a marked forward convexity, whilst the outer third of the bone is flattened from before backwards and shows a concave anterior border. At the outer end of the bone a slight elevation can usually be felt on the superior surface, and immediately external to this is the acromioclavicular joint, the long axis of which lies in the anteroposterior direction.
The acromial spine is narrow at about its centre, broadening out towards the vertebral border of the scapula, (Fig. XIII, 1.) and forming there a smooth triangular surface, over which glides the tendinous part of the trapezius. Externally, the spine terminates in the upward curved acromial process, (Fig. XIII, 2.) at the anterior border of which an oval facet is situated for articulation with the clavicle. The supra- and infraspinatus muscles fill up the depressions or fossae which lie in relation to the spine of the acromion.
The clavicle is also bounded above and below by depressions, little evident in fat subjects, but most marked when, as the result of pathological or physiological conditions, fat is feebly represented. The supra-clavicular (Fig. IV, 18.) or subclavian triangle is dealt with in the first chapter. The infraclavicular space is bounded above by the clavicle, below by the clavicular head of the pectoralis major muscle, internally by the costal cartilage of the first rib, and externally by the anterior border of the deltoid muscle. The floor is formed by the subclavius muscle and the costo-coracoid membrane. In the outer part of the space the coracoid process may be felt, (Fig. VI, 3.) the apex of the process lying under cover of the anterior border of the deltoid muscle. In favourable cases, the pulsation of the axillary artery (Part I.) may be detected below the clavicle, as this vessel runs downwards from the outer border of the first rib. The bulky deltoid muscle,(Fig. XIV, 5.) arising from the clavicle and from the acromial process and spine, is, so to speak, pushed outwards by the underlying head and great tuberosity of the humerus, so producing the normal rounded appearance of the shoulder. This outward displacement of the muscle is taken advantage of by Hamilton in the diagnosis of a dislocation of the shoulder-joint, as, after such an injury, the humerus is drawn inwards by the pectoralis major, latissimus dorsi and other muscles to such a degree that a ruler placed along the outer side of the arm will be in contact with the acromion process and the external humeral condyle at one and the same time. In the normal condition, this is not possible.
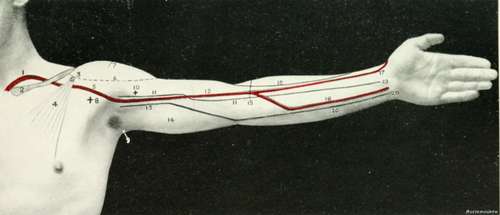
Fig. VI. The Front Of The Arm And Forearm
1. The subclavian artery.
2. The clavicle.
3. The coracoid process, 4. The pectoralis minor.
5. The axillary artery. 6. The anterior border of the deltoid.
7. The circumflex nerve and arteries.
8. The anterior axillary fold.
9. The posterior axillary fold.
10. The coraco-brachialis prominence.
11. The median nerve in the arm.
12. The brachial artery.
13. The ulnar nerve in the arm.
14. The triceps muscle.
15. The level of the head of the radius.
16. The radial nerve.
17. The radial artery.
18. The ulnar artery.
19. The median nerve in the forearm.
20. The ulnar nerve in the forearm.
To measure the length of the humerus, the tape-measure Fig. XIV, 4, should be carried from the lower margin of the acromial process to the external condyle of the humerus. The lesser tuberosity of the humerus is always difficult to identify, but it can usually be distinguished lying rather below the mid-point of a line uniting the coracoid process and the great tuberosity of the humerus, the arm being well everted and the elbow in contact with the side of the body.
Between the two tuberosities is the bicipital groove, in which runs the long tendon of the biceps muscle. The groove may be represented by a line, about 2 inches long, which runs downwards from the tip of the acromial process, parallel to the long axis of the humerus.
The upper epiphysis of the humerus includes the head and both tuberosities, and the epiphysial line runs transversely, at right angles to the long axis of the humerus, at the lower border of the great tuberosity.
Continue to:
- prev: The Brachial Plexus
- Table of Contents
- next: The Axilla