Lower Jaw Or Mandible. Part 3
Description
This section is from the book "The Anatomy Of The Human Skeleton", by J. Ernest Frazer. Also available from Amazon: The anatomy of the human skeleton.
Lower Jaw Or Mandible. Part 3
The small masseteric artery runs to the coronoid notch between the bone and the
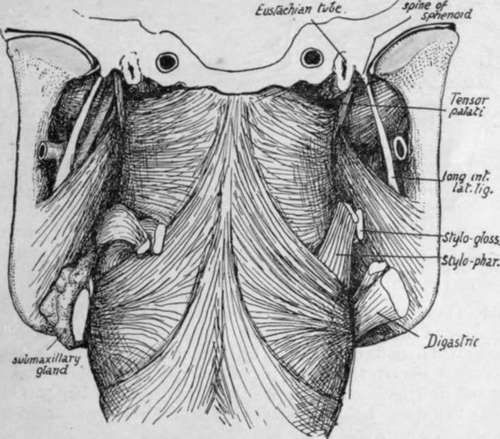
Fig. 205.-To show the deep relations of the lower jaw and its muscles. The pharynx, with the jaw in position, is seen from behind. On the right the Digastric, Stylo-hyoid, Stylo-pharyngeus, and Stylo-glossus are cut short: on the left the last two muscles are turned back, and the submaxillary gland is shown between the internal pterygoid and Digastric and Stylohyoid, and above them. The parotid, with a quantity of loose tissue, occupies the interval above and behind the Pterygoideus internus.
External Pterygoid, and passes immediately behind the Temporal tendon : its course below the outer Pterygoid is thus different from that of the masseteric nerve, which is above the muscle, between it and the base of the skull (see Fig. 182), and is therefore not a relation of the mandible.
The Temporal insertion is on the edge of the coronoid process, from the bottom of the notch almost to the alveolus ; it only extends slightly on to the surfaces of the process, usually more so on the inner than on the outer side.
The roughness of the masseteric area indicates that it also has tendinous fibres at its insertion. Observe that the area of insertion extends very high ; this is for the attachment of the more vertical posterior fibres, which have little play in the normal opening of the mouth and can therefore be fastened nearer their origin. The fibres that have most movement and more powerful action arise from the malar further forward and are directed downwards and backwards to the lower part of the ramus.
The upper part of the posterior margin of the ramus slopes back into the neck. Thus a triangular area of bone is exposed behind the level of the margin of the Masseter, and the parotid gland comes into relation with the bone here, being otherwise separated from its outer surface by the muscle. The gland also lies in contact with the border of the ramus, turning round it deeply to come into relation with the inner aspect and with the Internal Pterygoid, and the lower and deep part of its capsule is thickened to form the " stylo-mandibular ligament " which is attached to the lower part of the posterior margin.
The temporo-mandibular joint is a complex one, divided by an interarticular fibro-cartilage into two distinct cavities. The outer edge of the neck of the bone presents a ridge for the attachment of the external lateral ligament, the fibres of which are directed downwards and backwards from the eminentia articularis (Fig. 204). On the inner side another ridge marks the short internal ligament ; both these are thickened parts of the capsule. The capsule is very thin behind, but thicker in front where it receives some fibres of the External Pterygoid : it is attached all round the periphery of the fibro-cartilage, so that the menisco-mandibular and menisco-squamous cavities are quite distinct.
The fibro-cartilage fits on the articular eminence and in the articular cavity so that its upper surface is concavo-convex, while its lower surface is deeply concave to rest on the condyle of the mandible. The head of the mandible can plainly only rotate in the lower cavity, whereas the menisco-squamous joint is evidently only capable of a sliding movement.
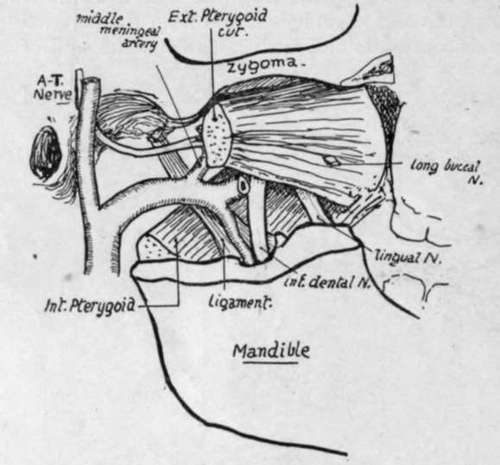
Fig. 207.-To show the structures lying in relation with the lower jaw above the level of the inferior dental foramen. For comparison with Figs. 204 and 206.
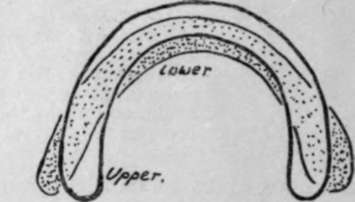
Fig. 20S.-To illustrate the different curves of the dental arcades in upper and lower jaws; lower arcade is shaded.
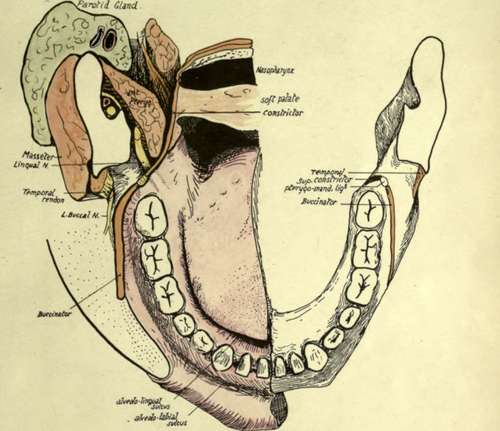
Fig. 206.-Diagram to show the relation of the mucous membrane and the wall of the pharynx to the mandible and its muscles.
A little consideration will show that it would be impossible to open the jaw wide if it rotated on an axis going through the temporal articulation, for the parotid and Sterno-mastoid would prevent any large movement of the angle backwards : this difficulty is overcome by putting the axis of rotation further down, when the jaw can be widely opened with half the amount of movement backwards of the angle but with a proportionate movement forward of the upper end. In such action the fixed point or axis of rotation is at the attachment of the long internal ligament : the foramen for the entering nerve and vessels is associated with this point, so that they enter the bone at its point of least movement. Some are inclined to place the position of the axis of movement lower still, at the attachment of the stylo-mandibular ligament. The External Pterygoid * starts the movement of opening by its contraction, thus drawing forward the fibro-cartilage as well as the head of the bone, so that the latter always has a hollow cavity in which it can turn : the forward movement of the bone with its depression (caused by its head being carried on to the eminentia articularis) tends to tighten the long ligament, and further action of the outer Pterygoid can only pull the upper end of the bone forward on the axis passing through the lingula. The long internal lateral ligament is attached to the lingula and the whole length of the adjoining margin of the foramen ; it is fastened above to the spine of the sphenoid, which is on the inner border of the glenoid cavity. The short internal ligament is attached to the base of the sphenoidal spine, and the line of the rest of the capsule runs round the articular surface on the squama of the temporal. The auriculo-temporal nerve runs back between these two ligaments (Fig. 182). The condyle projects markedly inwards, and the neck exhibits a corresponding widening from side to side as it passes up to support the head : the wide part is concave in front, gives attachment to the front part of the capsule and, below this, to the
Continue to: