Total Infiltration Of The Stomach
Description
This section is from the book "Cancer And Other Tumours Of The Stomach", by Samuel Fenwick. Also available from Amazon: Cancer and other tumours of the stomach.
Total Infiltration Of The Stomach
This condition is very rare, and is met with in less than 3 per cent, of all cases. When the morbid growth is fibrous in character the stomach becomes greatly reduced in size and presents the appearance of a leather bottle; but the soft spheroidaland cylindrical-celled carcinomata produce a greater thickening of the gastric wall with a lesser diminution of lumen. In the former case the disease may run a protracted course, and is often unaccompanied by metastases, while in the latter death occurs at an earlier period, and is usually accelerated by secondary growths of the peritoneum or liver.
For several months the chief symptoms consist of discomfort, flatulence, and distension after meals, with anorexia, loss or flesh, debility, anaemia, and constipation. As soon as the greater part of the stomach has been involved, or one of the orifices is contracted, vomiting becomes the most prominent feature, and increases in severity until the end. At first it chiefly ensues after the ingestion of an unusually large meal, when the patient feels that he has overtaxed the capacity of his stomach and rejects the surplus amount as an infant does under similar circumstances. Gradually the quantity of food has to be reduced, until less than six fluid ounces can be swallowed without producing regurgitation. About this period attacks of acute gastritis are apt to supervene, and to give rise to continuous retching and vomiting, which prevent the administration of food by the mouth. When these acute symptoms subside the general health is found to have greatly deteriorated and the power of absorption to be much impaired. The final stage of the disease is characterised by the regurgitation of food immediately after it has been swallowed, and a complete inability to partake of solids. These symptoms so closely resemble those that ensue from obstruction of the oesophagus that they frequently lead to an erroneous diagnosis.
In some cases the symptoms are gradually engrafted upon those of pyloric stenosis, owing to the extension of what was originally a localised growth. In these circumstances the periodic vomiting becomes more frequent, more immediately dependent upon the ingestion of food, and less profuse, until the amount of nourishment that can be taken becomes greatly reduced and regurgitation occurs immediately after swallowing. When a growth that originally obstructed the cardia progressively involves the walls of the stomach until it produces a general contraction of the organ, the initial dysphagia and regurgitation continue throughout the whole course of the complaint.
Pain is chiefly experienced when the mucous membrane undergoes superficial ulceration or the serous coat becomes inflamed and adherent to the surrounding organs. In the former case the ingestion of solid food, or even milk, gives rise to an aching or burning sensation at the epigastrium, which is relieved, though not removed, by vomiting; while in the latter constant and severe pain develops without obvious cause, and continues with a varying intensity for many weeks.
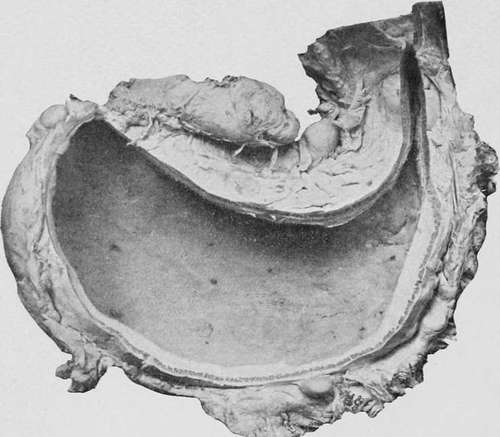
Fig. 52.-A stomach viewed from behind, , with enlarged glands along the curvatures. (Museum of the Royal College of Surgeons.).
Cachexia is a marked symptom when pain is the predominant feature of the complaint, and is usually attributed to exhaustion. It may often be observed, however, that the vomit constantly contains small quantities of altered blood, or that signs of haemorrhage are unexpectedly discovered when the stomach is emptied by a tube. The duration varies according to the rapidity of infiltration and the degree of contraction of the stomach. Of the cases we collected from different sources the average was ten months, while of those contained in our own series 50 per cent, lived more than a year and 12 per cent, more than eighteen months.
The Physical Signs differ somewhat from those of the other varieties of the disease. Instead of presenting evidences of dilatation, the stomach becomes progressively smaller, and towards the termination of the complaint may be quite obscured by the intestines. Owing to rigidity of the gastric walls it is impossible to inflate the organ, and the gas that is introduced immediately escapes into the oesophagus or bowel. The employment of a tube is apt to confuse rather than to aid the diagnosis, since the contracted state of the stomach offers resistance to the passage of the instrument, and consequently may simulate a stricture of the oesophagus. It may usually be observed, however, that the apparent stricture is situated at a distance greater than eighteen inches from the incisor teeth, and that the fluid extracted is acid in reaction. After the administration of a test meal only a small quantity of material can be withdrawn, and from the filtrate both free hydrochloric and lactic acids are found to be absent. When vomiting is excessive the gastric fluid is usually alkaline. In about one third of the cases a rounded irregular or elongated tumour may be detected in the epigastrium or left hypochondrium, which moves with respiration and may sometimes be felt to harden and relax alternately when grasped bv the hand.
Continue to: