Carcinoma Of The Cardia
Description
This section is from the book "Cancer And Other Tumours Of The Stomach", by Samuel Fenwick. Also available from Amazon: Cancer and other tumours of the stomach.
Carcinoma Of The Cardia
The cardiac third of the stomach is primarily affected in about 10 per cent, of all cases, and is more frequently involved in men than in women. As a rule the previous health has been extremely good, but occasionally the onset of the disease is preceded for some months by pyrosis. The first symptom to attract attention is usually a difficulty of swallowing, which is often attributed to soreness of the throat or to the ingestion of a fish-bone or other foreign body; but occasionally it develops quite suddenly and without apparent cause. Each mouthful of solid food appears to stick in the gullet, and. deglutition is accompanied by a sense of uneasiness, fulness, or of actual pain behind the lower end of the sternum. At the same time there is usually a complaint of want of appetite, loss of flesh, breathlessness on exertion, and debility, and sometimes of attacks of sharp pain in the left side of the chest and back. Gradually the dysphagia increases, until every attempt to swallow solids is accompanied by choking and regurgitation of the food, and even liquids are rejected unless taken slowly and in small quantity. These phenomena occupy from three to seven months in their development, at the end of which period the patient presents a pallid, careworn, and starved appearance, and is found to have lost between two and three stones in weight. The symptoms of the final stage vary in different cases. Severe haemorrhage is rare, but not infrequently the ejecta consist of grumous material or exhibit streaks or clots of bright blood.
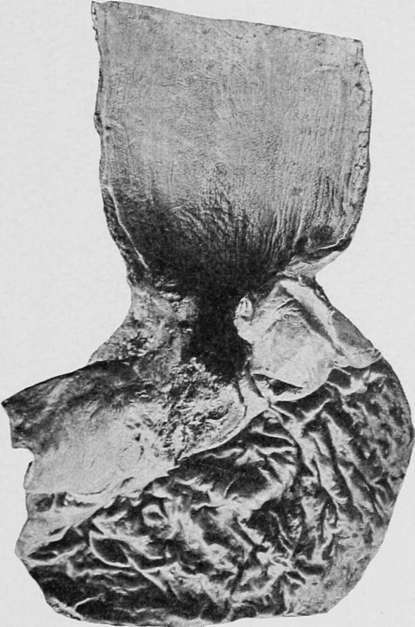
Fig. 48.- situated at the cardiac orifice and spreading into the oesophagus. (London Hospital Museum.).
In most instances increasing debility compels the patient to keep his bed, and he gradually succumbs to asthenia. In other cases delirium supervenes, the mouth and throat are attacked by thrush, and death ensues from exhaustion, secondary pneumonia, or from septic absorption from the dilated oesophagus. Perforation of the stomach is rare, but sometimes sloughing of the oesophagus gives rise to empyema, pneumothorax, or gangrene of the left lung. Occasionally ulceration of the growth removes the obstruction, so that food can once more be swallowed with comparative ease. Death usually occurs within nine months.
When the disease affects the cardiac region or the fundus, without involvement of the oesophagus, dysphagia is absent and the principal symptoms are those of dyspepsia. Pain is almost always present, and is chiefly experienced immediately after a meal containing solid food, but it may also be provoked by hot liquids, or even by milk. Vomiting occurs in the majority of cases, but affords little relief to the pain. Slight haematemesis is also a frequent symptom, but owing to the integrity of the pylorus the blood is more often bright-red than altered by its retention in the stomach. Anorexia, loss of flesh, and cachexia are prominent symptoms, and diarrhoea often alternates with or replaces the usual constipation. Life is rarely prolonged more than a year, and death usually occurs from exhaustion, aggravated by secondary disease of the liver or peritoneum.
Stenosis of the cardiac orifice may be recognised by the resistance offered to the passage of a soft tube at a spot about 16-18 inches (40-47 cms.) from the incisor teeth, and by the evacuation in the eye of the instrument of a small quantity of undigested food which had accumulated above the stricture. Examination of the latter shows it to consist of alkaline mucus and saliva, mixed with milk and particles of food, and occasionally with pus or blood ; while the microscope reveals the existence of salivary corpuscles, blood-cells, and sometimes of small portions of the neoplasm detached by ulceration. Auscultation over the epigastrium demonstrates a considerable delay, or even suppression, of the second deglutition sound, which under normal circumstances may be heard in seven to twelve seconds after the patient has swallowed a mouthful of fluid. The disease is rarely accompanied by a palpable tumour, though occasionally the contracted stomach forms an elongated or rounded swelling, which can be felt between the ensiform cartilage and the left costal margin.
Carcinoma of the fundus is usually associated with a nodular tumour, which occupies the left epigastrium or hypochondrium, descends upon inspiration, and is susceptible of slight lateral displacement. The stomach itself is often smaller than normal, and in 68 per cent, of the cases its contents after a test meal are found to be free from hydrochloric acid and to exhibit an excess of lactic acid. At a late stage the omentum and the left lobe of the liver often present metastases, and the glands above the left clavicle may become enlarged. When the disease gives rise to a stricture near the centre of the organ, the symptoms resemble those of pyloric stenosis, and examination shows considerable dilatation of the fundus without a palpable tumour.
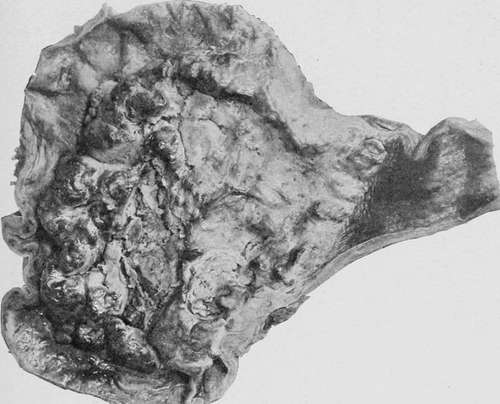
Fig. 49.- involving the greater part of the stomach and extending into the oesophagus. (Museum of the London Temperance Hospital.).
Sizzling and gurgling sounds may sometimes be heard over the epigastrium.
Continue to:
- prev: Chapter VII. Clinical Varieties
- Table of Contents
- next: Carcinoma Of The Body (Walls And Curvatures)