Operation Of Tying The Axillary Artery In Its First Stage
Description
This section is from the book "Anatomy Of The Arteries Of The Human Body", by John Hatch Power. Also available from Amazon: Anatomy of the Arteries of the Human Body, with the Descriptive Anatomy of the Heart.
Operation Of Tying The Axillary Artery In Its First Stage
The operations is extremely difficult, from the depth of the artery, and the difficulty of distinguishing it from the adjacent nerves of the brachial plexus, and on account of the situation of the axillary vein and the probable occurrence of troublesome venous hemorrhage; for these reasons the ligature of the subclavian, in its third stage, is generally preferred for the cure of axillary aneurism. The following mode of operating is essentially the same as that recommended by Mr. Hodgson. The patient should be seated in a reclining chair, or laid on a table, so as to let the light fall on the site of the operation. The arm being abducted, a semilunar incision should be next made, commencing within an inch of the sternal end of the clavicle, and stopping short externally at the edge of the deltoid muscle, in order to avoid injuring the cephalic vein. This incision will have its convexity turned downwards, and will divide the integuments and platysma myoides. The fibres of the great pectoral muscle should then be divided in the same manner, and to the same extent. On retracting the lips of the wound, the pectoralis minor muscle will be seen crossing it inferiorly. This muscle may now be relaxed, by bringing the arm nearer to the side, and should then be depressed with a blunt instrument, so as to give more room to the operator. By cautiously scraping through the areolar membrane, the acromial artery will be found projecting over the edge of the muscle, and will assist in guiding us to the axillary artery: the costo-coracoid ligament may be divided, if necessary, on a director. We should remember that the anterior thoracic nerve is in front of the artery; the brachial plexus above and to the outside of it; and the vein, which often swells suddenly out in front of the artery during expiration, is on a plane anterior and internal to it. Having found the artery, the needle must be passed round it, from within outwards, in order to avoid injuring the vein, which should be drawn inwards with a blunt hook or a curved spatula. Before tightening the ligature, we should ascertain that compression of the included part restrains the pulsation of the aneurismal tumor.
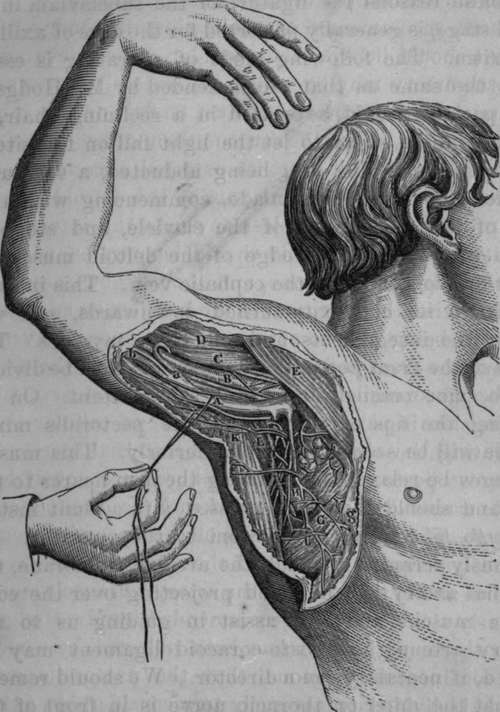
Fig. 24. Surgical Anatomy of the Axillary Artery in part of its course.
A, Axillary Vein drawn downwards. The Internal Cutaneous Nerve crosses the rein, and one of the nerves of Wrisberg is In immediate relation with it internally. B, Axillary Artery crossed by one of the roots of Median Nerve. C, Coraco-brachialis Muscle. D, Biceps Muscle. E, Pectoralis Major Muscle. F, Pectoralis Minor Muscle. G, Serratus Magnus Muscle. H, An Axillary gland crossed by a branch of the External Respiratory Nerve. I, Infra or Subscapular Artery. K, Latissl-mus Dorsi Muscle. L, Teres Major Muscle, a. Trunk formed by Venae Comites. b, Basilic Vein assisting in forming the Axillary Vein, g, Fascia.
Manec recommends the following method :" The patient should lie "with the shoulder rather elevated, so that the artery may be a little separated from the vein; to attain this end the elbow must be four or five inches apart from the body: the surgeon then makes an incision two or three inches long, its external extremity commencing upon the internal part of the deltoid muscle, and prolonged more or less towards the internal extremity of the clavicle; it should be parallel with the anterior edge of that bone, and about eight lines below it. In giving this direction to the incision, an advantage arises in being able to arrive directly upon the vessels and nerves from before backwards, so that the artery can be more easily insulated ; on the contrary, when the incision is parallel with the layer of cellular tissue separating the clavicular from the sternal portion of the great pectoral, it is true its fibres are not divided, but the wound does not correspond with the direction of the artery." The remaining steps of the operations consist in the transverse division of the fibres of the greater pectoral and in the tying of the artery. Manec's method is nearly similar to that recommended by Mr. Hodgson.
To these methods it has been objected, by some of the continental surgeons, that the pectoralis major muscle is divided transversely to a considerable extent, and the shoulder thereby considerably weakened; they, therefore, prefer an incision in the course of its fibres, and separating its clavicular from its sternal portion. The objection to the transverse division of the fibres of the great pectoral is more fanciful than real, whilst there is a decided objection to the plan of coming down upon the artery by cutting between the clavicular and sternal origins of the pectoralis major muscle,viz. that this incision will conduct us more directly upon the vein than upon the artery.
The operations of tying the Axillary artery in its second stage has been recommended by Delpech : he divides the pectoralis minor muscle and thus secures the artery in this stage. He has in this way twice taken up the artery successfully for hemorrhage after amputation.*
Continue to:
- prev: Third Stage Of The Axillary Artery
- Table of Contents
- next: Operation Of Tying The Axillary Artery In Its Third Stage