Direct Invasion
Description
This section is from the book "Cancer And Other Tumours Of The Stomach", by Samuel Fenwick. Also available from Amazon: Cancer and other tumours of the stomach.
Direct Invasion
The fact that a morbid growth invariably invades the submucous tissue for some distance beyond its apparent confines suggests that it would frequently extend by continuity into the oesophagus or duodenum. As a matter of fact, however, such a process is comparatively rare as compared with the invasion of merely contiguous structures. Thus, out of the 131 cases already referred to, we find that the pancreas was directly invaded in twenty-two, or 16.7 per cent. ; the liver in eighteen, or 13.7 per cent.; the colon in seven, or 5.3 per cent.; the spleen in five, or 3.7 per cent.; the oesophagus in eight, or 4.5 per cent.; and the duodenum in two, or 1.5 per cent. The preference thus exhibited to invasion via the peritoneum probably depends upon the peculiar facilities which the latter affords, by its extensive system of lymphatics and by the numerous bridges which exist, in the form of fibrinous adhesions, for the transference of cancer cells from one organ to the other. The exceptional liability of the pancreas is probably the result of three allied conditions. In the first place, its situation immediately behind the stomach not only brings it into close contact with almost every growth which affects that viscus, but also with those species (medullary and adeno-carcinomata) which possess the greatest degree of malignancy. Again, the firm structure of the gland and its fixed position greatly conduce to the formation of adhesions and to their subsequent invasion by the disease. Finally, the close proximity of the coeliac glands and of the great lymphatic vessels which drain the lower half of the stomach must always be a source of considerable danger to the organ.
The situation of the liver renders it less exposed to direct invasion, since it only comes into contact with the upper margin and a part of the anterior surface of the stomach, while its constant movement during respiration militates against the formation of adhesions. These natural advantages are, however, more than counterbalanced by its connection with the lesser omentum and the vessels it contains, since these constitute a means of communication with the diseased stomach, of which the neoplasm only too often takes advantage.
The spleen is much less frequently invaded than the aforementioned organs, owing to its remote situation from the usual seat of disease and to the peculiar distribution of the gastric lymphatics. If, however, only those cases are examined in which the growth affects the cardiac end of the stomach, this disparity at once disappears (vide Table 7, p. 56). For a similar reason the transverse colon is only directly implicated in about 5.3 per cent, of all cases of gastric cancer, but in nearly 32 per cent, of those in which the great curvature is the seat of the primary growth. Direct invasion of the kidney is very rare; but a similar immunity is not shared by the suprarenal glands, which are frequently involved (especially the left one) in disease of the posterior surface of the stomach and of the cardia.
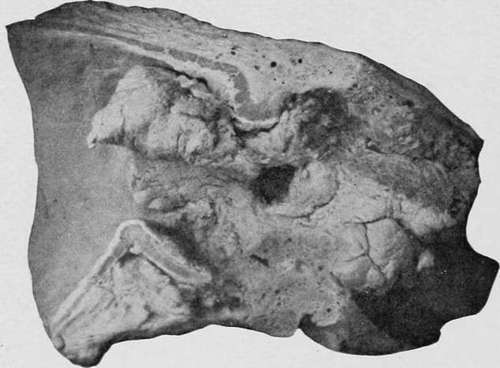
Fig. 26.-A large growth of cylndrical-celled carcinoma at the pylorus, extending into the duodenum. (Museum of the Royal College of Surgeons.).
Turning now to the question of invasion by continuity, it is at once obvious that a great difference exists between the respective liability of the duodenum and the oesophagus. A pyloric growth, if it spreads at all, almost always extends in the direction of the body of the viscus, and though it may actually project into the lumen of the duodenum, but rarely implicates its walls. Lebert observed one exception to this rule in the course of thirty-four necropsies upon cancer of the pylorus, Brinton ten in 125, and ourselves two in eighty-seven. Thus, out of a total of 246 pyloric growth involved the duodenum in only thirteen, or 5.2 per cent. It also seems that the cylinder-cell variety more often affects the bowel than the other forms.
On the other hand, the natural tendency for a cancer of the cardia is to spread into the walls of the oesophagus. When the disease develops in the immediate vicinity of the orifice, this mode of extension probably occurs in every case (Bokitansky) ; but when it primarily implicates the walls or curvatures at some distance from the aperture, we find that invasion of the oesophagus takes place only in about one-half of the cases (46 per cent.).
The notable difference which is thus observed in the spread of a neoplasm at opposite ends of the organ is best explained by contrasting the mode of insertion of the oesophagus into the stomach with that of the pylorus into the duodenum. In the former case the submucous and muscular coats of the two viscera are perfectly continuous, and there is, consequently, no obstacle to the spread of a morbid growth from one organ to the other. The duodenum, on the other hand, is attached to the pylorus much in the same way as the vagina embraces the neck of the uterus, the submucous and the inner and muscular coats of the two viscera along the line of fusion being so distinct from one another that direct continuity can scarcely be said to exist. It consequently happens that a growth of the pylorus is more apt to infiltrate the contiguous walls of the stomach than to extend obliquely along a comparatively thin and external layer of tissue into the wall of the bowel. It is also probable that the lymphatic vessels of the pylorus, by pursuing a course away from the bowel towards the cardia or the pancreas, also tend to promote extension of the disease in an opposite direction to the duodenum.

Fig. 27.-A soft spheroidal-celled growth of the cardiac orifice extending up the oesophagus. (London Hospital Museum.).
The appearances presented by the organs directly invaded by carcinoma vary considerably in different cases. When the pancreas is affected the whole or greater portion of the gland is usually destroyed; but in the case of the liver and spleen the disease more often takes the form of a globular or wedgeshaped mass, which extends only a short distance into their interior, but is accompanied by great infiltration of the subserous tissue and lymphatic glands. Extension to the colon takes place through the medium of the gastro-colic omentum and newly formed adhesions, and not infrequently gives rise to a large mass of growth between the stomach and the bowel, which greatly obstructs the lumen of the latter. Invasion of the oesophagus occurs most frequently in soft spheroidal-celled cancers, and either affects the entire circumference of the tube for half an inch or more above the cardiac orifice, or produces an irregular infiltration of its posterior and inner wall. This latter variety often leads to perforation. More rarely the submucous tissue of the oesophagus is invaded by one or more series of nodules, which extend for some distance in its longaxis and may even reach the pharynx (Lazarus-Barlow). These occasionally ulcerate and produce small circular sores. When the disease invades the duodenum it seldom involves more than two inches of the bowel.
Continue to: