The Thoracic Cavity
Description
This section is from the book "Surgical Anatomy", by John A. C. MacEwen. Also available from Amazon: Surgical Anatomy.
The Thoracic Cavity
The Thoracic Cavity contains the lungs, which are separated by the mediastinum, containing the heart, vessels, trachea, etc. The mediastinum extends from the sternum to the spine, forming a complete septum between the lungs, and is deflected somewhat toward the left. It is bounded by the diaphragm below, but is open above, while laterally it is bounded by the pleurae. Its upper part contains the aortic arch and great vessels, innominate veins, and upper portion of the superior vena cava ; trachea, oesophagus and thoracic duct; phrenic, pneumogastric, left recurrent laryngeal and cardiac nerves ; and thymus gland. The lower part is chiefly occupied by the heart and pericardium and phrenic nerves placed centrally. In front of the pericardium and behind the gladiolus the mediastinum is practically non-existent in its upper se-gment, owing to the pleurae coming in contact, but below the fourth costal cartilage the pleurae diverge. This anterior portion contains areolar tissue and lymphatic glands and vessels. Behind the pericardium the lower mediastinum communicates with the upper, and contains the descending thoracic aorta, azygos veins, oesophagus, thoracic duct, and two pneumogastric nerves. The azygos veins commence below in the lumbar veins, and communicate with the iliacs, renals, etc. ; receive blood from the intercostal veins ; and discharge into the superior vena cava. They may be of great assistance where the main trunk is obliterated, and when themselves pressed on tend to cause oedema of the chest-wall from engorgement of the intercostal veins. The mediastinum is sometimes the seat of abscesses which may develop from the contained glands or the dorsal vertebrae, or may extend to it from the neck. Such abscesses are generally chronic, and become of large size, pressing upon the trachea, bronchi, or oesophagus. Sarcomatous tumours and aortic aneurism also give rise to pressure symptoms, the effects on the veins being often particularly obvious, the face, neck, and upper limbs becoming ©edematous from pressure on the superior vena cava, and innominate, while the veins of the trunk also become distended from the increased flow of blood through them. The vagus, recurrent laryngeal, and sympathetic nerves also become affected.
The fibrous pericardium, of inverted conical shape, is attached above to the roots of the great vessels, and below to the central tendon of the diaphragm. Laterally and anteriorly it is bounded by the pleurae, while posteriorly it is largely free. Above, the fibrous pericardium is lost upon the great vessels about the level of the centre of the manubrium, whence, however, it becomes connected with the pretracheal layer of the deep cervical fascia (cervico-pericardiac fascia). This connection between larynx, pericardium, and diaphragm explains why the larynx descends slightly on inspiration. Below, owing to the base sloping downwards and forwards to the left, it has indirect relationships to the left lobe of the liver and upper wall of the stomach. This latter relationship helps to explain the cases of fainting which sometimes occur from flatulent distension of the stomach pressing directly upon the heart. The lower extremity of the thymus gland rests upon the upper portion of the anterior surface, and a small portion of this anterior surface to the left of the middle line, and behind the sternum and fourth, fifth, and sixth ribs, comes into relationship with the chest-wall. The posterior surface is related to the thoracic aorta and duct, the oesophagus and vagi nerves, and the bifurcation of the trachea. Within the fibrous pericardium is the serous pericardium, which, like the peritoneum, is a closed sac containing a little fluid, the parietal layer of which invests the inner surface of the fibrous layer, while the visceral partially ensheaths the heart and great vessels. The aorta and pulmonary artery are enclosed together in a complete sheath of visceral layer, which is separated from the auricles, which lie in front, by a passage, called the great transverse sinus, running from right to left. The other vessels receive partial coverings, and also present sinuses separating them from the serous pericardium. The pericardium may be occupied by a considerable amount of fluid without pressing unduly upon the heart, the sac stretching, if time be given it, at the expense of the lungs, the above-mentioned sinuses, etc. In such cases the pericardium has been known to contain fully 2 pints of fluid, the superficial area of heart dulness being increased, and the heart, which has its root in the great vessels, being pushed upwards and backwards, its impulse becoming imperceptible, and the diaphragm being depressed. In examining such conditions it is important to know the normal relationship of the anterior surface of the heart to the chest-wall. The projection of the anterior surface, then, may be defined by four lines-aoove, across the sternum just above the upper borders of the third costal cartilages, and extending beyond it for ½ inch on the right and 1 inch on the left ; below, from a point on the right sixth costal cartilage, ¾ inch from the sternal margin, downwards to the left fifth intercostal space, 3½ inches from mid-sternum (this latter point represents the position of the apex) ; on the right, from the extremities of the top and bottom lines, in a curve with the convexity outwards, which reaches at the level of the fourth costal cartilage, a point 1½ inches from the mid-sternal line ; on the left, also curved with the convexity outwards, and joining the extremities of the top and bottom lines. A small triangular portion of the heart, chiefly right ventricle, is left uncovered by lung, and is defined by drawing a vertical line along the mid-sternum from the lower border of the fourth costal cartilage to the junction of the gladiolus and xiphoid, and joining either extremity of this with the apex in the fifth intercostal space. Where effusions come on rapidly, serious consequences may follow even comparatively slight accumulations, and in such cases it may be necessary to tap the pericardium, or, where the fluid is purulent, to drain it. Tapping is best done through the sixth left intercostal space, keeping close to the sternum, so as to avoid the internal mammary artery. The space is narrow, and the needle should not be introduced much more than an inch, lest the heart be wounded. Where it is necessary to open up the pericardium (pericardotomy) for draining or stitching cardiac wounds, a vertical incision along the left margin of the sternum, from the fourth to seventh costal cartilage, is made, and the sternum and cartilages exposed. The fifth cartilage is first cut close to the sternum, and then raised, the underlying tissues being carefully reflected from it, so as to avoid the internal mammary artery, and a piece cut out. The sixth cartilage is similarly treated. Then the triangularis sterni muscle is incised vertically, close to the sternal margin, the soft tissues carefully reflected, the pericardium exposed, picked up, and incised, also vertically, for about an inch, the pericardial edges being afterwards sutured to the subcutaneous tissues to prevent dissemination of purulent material. It should be remembered, however, in connection with operations on the pericardium, that the area left uncovered by the pleura varies, the left pleura occasionally overlapping practically the entire pericardium.
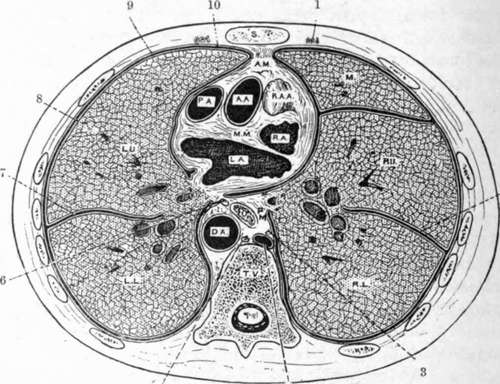
Fig. 18.-Transverse Section of the Thorax through the Second Sternebra in Front and the Body of the Ninth Thoracic Vertebra Behind, showing the Reflections of the Pleura and the Position of the Viscera.
s. | Sternum. | P.M. | Posterior mediastinum. |
A.M. | Anterior mediastinum. | O. | |
A. A. | Ascending aorta. | D.A. | Descending thoracic aorta. |
P.A. | Pulmonary artery. | T.V. | Thoracic vertebra. |
R.A.A. | Right auricular appendix. | M. | Middle lobe of right lung. |
R.A. | Right auricle. | R.U. | Right upper lobe. |
M.M. | Middle mediastinum. | R.L. | Right lower lobe. |
L.A. | Left auricle. | L.U. | Left upper lobe. |
L.L. | Left lower lobe. | ||
1. | Internal mammary vessels. | 6. | Left vagus nerve. |
2. | Right chief pulmonary fissure. | 7. | Left pulmonary fissure. |
3. | Right vagus nerve. | 8. | Pulmonary pleura. |
4. | Right azygos vein. | 9. | Pleural interval. |
5. | Thoracic duct. | 10. | Parietal pleura. |
Continue to:
- prev: The Mammary Gland
- Table of Contents
- next: The Heart