Microscopic Examination. Part 6
Description
This section is from the book "Cancer Of The Stomach", by A. W. Mayo Robson, D.Sc, F.R.C.S.. Also available from Amazon: Cancer of the Stomach.
Microscopic Examination. Part 6
Tea.-Bread and butter or a little toast, one cup of tea.
8 p.m.-Cup of milk and one tea-spoonful of plasmon.
Supper.-Nearly one pint of boiled milk and bread.
In 1906, over five years after operation, he was seen by the matron of the surgical home where he sta}Ted, and she reported him as looking in robust health and of normal weight. He was again reported well in 1907.
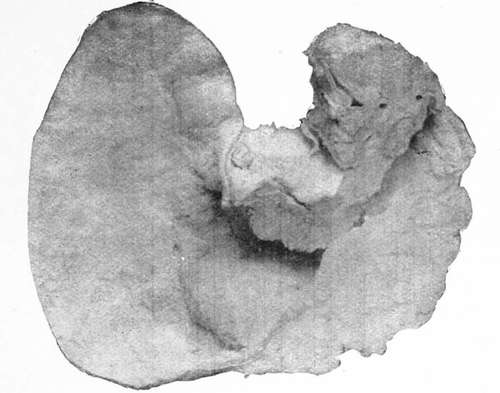
The tumour removed was a nodular, softish growth, involving almost the whole of the stomach, including the pylorus and extending from it to the cardiac end, where a small margin of healthy stomach wall remained. It weighed 1 lb. immediately after operation. Unfortunately the specimen, which was sent to a pathological laboratory to be mounted and reported on, was mislaid and cannot be found. It is impossible, therefore, for me to say whether it was sarcoma or cancer, but from the absence of enlarged glands, from the rapidity of growth and from its freedom from adhesions I suspect that the growth was a sarcoma.
It was undoubtedly malignant and was invading the stomach walls generally; the growth was breaking down on its visceral aspect, and the stomach cavity contained some grumous material thrown off from the growth. The pylorus was invaded, but the line of section in the duodenum and at the cardiac end of the stomach showed a healthy appearance, and a free portion existed between the growth and the cut margin.
These cases out of others that I could relate will be sufficient to show that removal of even a considerable portion of the stomach may be something more than a palliative operation, and I think it justifies me in saying that although it is better to have cases of cancer diagnosed and operated on early, yet we need not take the pessimistic view which has been given by some surgeons that if a tumour be manifest it is too late to perform a radical operation.
I hope I have advanced sufficient evidence to prove :
(1) How desirable it is to make an early diagnosis of cancer of the stomach in order that a radical operation may be performed at the earliest possible moment.
(2) That it may be needful to perform an exploratory operation in order to complete or confirm the diagnosis.
(3) That such an exploration may be done with little or no risk in the early stages of the disease.
(4) That even where the disease is more advanced and a tumour perceptible, an exploratory operation is, as a rule, still advisable in order to carry out radical or palliative treatment.
(5) That where the disease is too extensive for any radical operation to be done the palliative operation of gastroenterostomy, which can be done with very small risk, may considerably prolong life and make the remainder of it much more comfortable and happy.
(6) That some cases, thought at the time to be cancer too extensive for removal, may after gastroenterostomy clear up completely and get quite well.
(7) That in cases of disease of the cardiac end of the stomach too extensive for removal the operation of gastrostomy may considerably prolong life and prove of great comfort to the patient by preventing death from starvation.
(8) That even where the disease is too extensive either for removal, or for a gastroenterostomy or even a gastrostomy being performed with a fair chance of success, the operation of jejunostomy may prove of service to the patient.
(9) That where a radical operation can be performed, the thorough removal of the disease may bring about as much relief to the patient as does the operation for removal of cancer of the breast, uterus, and other organs of the body, and that in some cases a complete cure may follow.
Cancer of pylorus, producing* stenosis, in a woman aged thirty-six.

Hour-glass stomach, possibly congenital, with growth round cardiac orifice.
Continue to:
- prev: Microscopic Examination. Part 5
- Table of Contents
- next: Chapter V. Simple Tumours Of The Stomach That May Be Mistaken For Cancer
Tags
stomach, operation, cancer, tumour, ulcer, gastric, gastrectomy