Abdominal Regions
Description
This section is from the book "Cancer Of The Stomach", by A. W. Mayo Robson, D.Sc, F.R.C.S.. Also available from Amazon: Cancer of the Stomach.
Abdominal Regions
I have found the method of artificially dividing the abdomen into four regions by two lines passing from the ninth costal cartilage to the opposite anterior superior spine to simplify for clinical purposes the surgical anatomy of the abdomen. We can thus speak of superior, inferior, right, and left abdominal regions as shown in the appended diagram.
Inspection should always precede other diagnostic efforts. The retracted, superior, abdominal region significant of starvation from oesophageal stricture; the rigid, immobile abdominal wall of incipient peritonitis ; the distension of the abdomen and the shallow breathing of general peritonitis; the sighing respirations in internal haamorrhage ; the irregular, catching breathing in diaphragmatic peritonitis or pleurisy due to subphrenic inflammation; the fixed and bulging ribs in subphrenic abscess; the tumour moving with respiration, often visible in cancer of the body or of the pyloric end of the stomach; the enormous bulging of the upper, or even of the whole abdomen in acute gastric dilatation; the visible peristalsis from left to right in obstruction at the pylorus, are among the many important points that may be revealed by inspection.
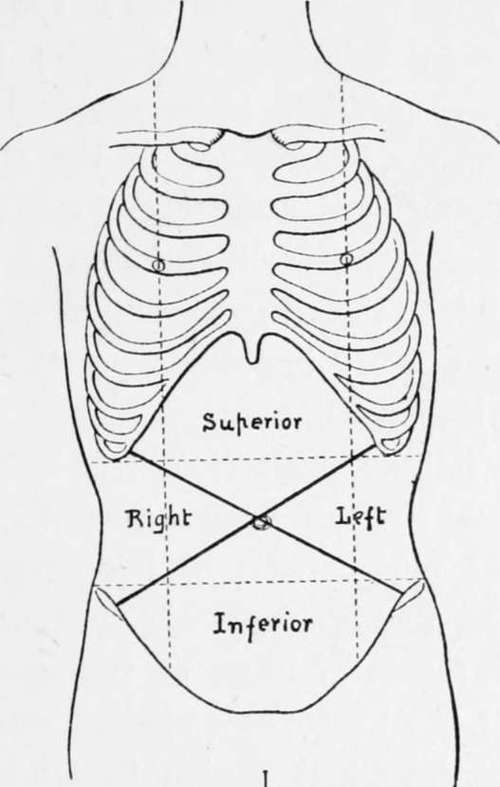
Fig. 2.
Palpation follows inspection, and is perhaps the method which we can least afford to omit. The rigid recti of perigastritis or incipient peritonitis; the fixed right rectus of pyloric or duodenal ulcer ; the fixed left rectus of ulcer at the cardiac end of the stomach : the tenderness elicited on pressure in the superior abdominal region in all inflammatory diseases and its absence in cancer ; the presence of a tumour, its nodular character, if malignant, and its mobility in the early stages ; the feeling of a peristaltic wave from left to right in mechanical obstruction at the pylorus ; the pylorus hardening under the hand in pyloric spasm, followed by a disappearance and then a re-appearance of the tumour; the general outline of the dilated stomach to be felt in acute gastric dilatation, or in a stomach artificially distended with gas or air; the occasional mapping out of an hour-glass stomach after artificial distension ; the differentiation between communicated and expansile pulsation in any tumour suspected to be aneurysm, and many other points can be almost definitely settled by palpation. Bimanual palpation with one hand in the loin and the other on the front of the abdomen will often add to the information concerning a tumour or other associated condition, as, for instance, a movable right kidney dragging on the pylorus, or a distended gall-bladder fixed by adhesions to the stomach.
Succassion is a modification of palpation frequently employed to elicit a stomach splash, which, if present habitually, usually indicates pathological dilatation, and which if present five to six hours after a full meal indicates motor inefficiency or some obstruction at the pylorus, or both. Leube's method of palpating a stomach-tube through the abdominal wall is, in my experience, not of material value.
In perforating ulcer, the presence of free fluid in the peritoneum may be ascertained by flicking the abdomen with the finger-nail during palpation, when a communicated wave may be felt. The same method is useful in ascertaining the presence of ascitic fluid, which if present along with a tumour of the stomach is usually indicative of advanced cancer.
The eliciting of certain tender spots by palpation on the surface of the body may be of great assistance ; for instance, tenderness in the superior abdominal region is suggestive of gastric ulcer and the site of tenderness to the left or right is some guide as to its position, especially when the rigidity of the corresponding rectus is taken into consideration. The most common site for tenderness in ulcer of the stomach is at the point marked on the diagram between the midline and the left costal margin; that for ulcer at the pylorus is usually on the right of the midline, and that for ulcer of the duodenum still more to the right and rather lower. In the dorsal region there are well-marked tender spots 1 to 2 in. to the left of the spine opposite the ninth, tenth, and eleventh ribs, which are present in many cases of ulcer.
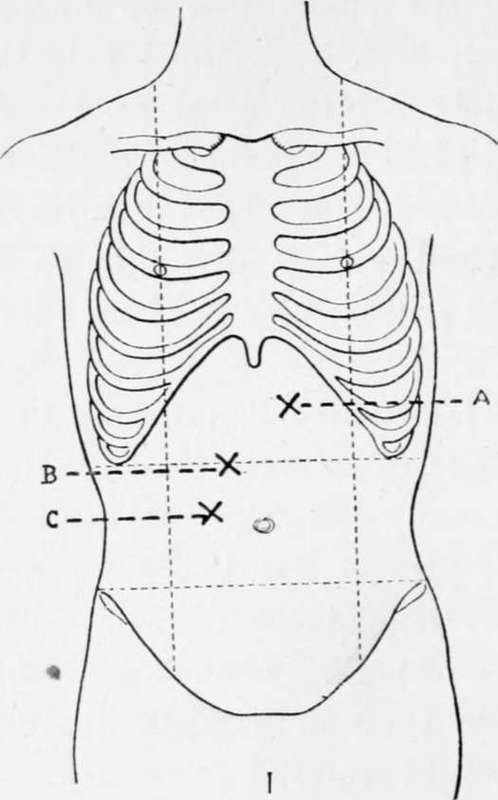
Fig. 3.-a. Usual site of tenderness in nicer of stomach. b. Usual site of tenderness in ulcer of pylorus, c. Usual site of tenderness in ulcer of duodenum.
Percussion is useful in ascertaining the size of the stomach, the resonance of which, when not distended with food under normal conditions should not reach below a point midway between the ensiform cartilage and the umbilicus, though stomach resonance reaching to the umbilicus does not necessarily mean the dilatation of disease. By means of percussion the size and shape of the stomach may be ascertained with the greatest accuracy, and in this way simple dilatation, dilatation of the dome of the stomach upwards, hour-glass deformity and gastroptosis may be readily demonstrated. It is more efficiently carried out after dilating the stomach, either with air pumped through a tube or by distending with carbonic acid gas, either by giving carbonate of soda and tartaric acid in water in successive doses, or by giving a tumblerful or two of soda water. If distension occurs after the administration of carbonate of soda alone, it usually indicates excess of acid in the stomach, which may point to hyperchlorhydria and ulcer. By percussion of the stomach with the patient upright, before and after drinking a measured quantity of water, the size and capacity of the stomach may be ascertained.
In the diagnosis between a gastric or a pancreatic tumour, light percussion will reveal resonance, but deep percussion dulness in pancreatic growth, this being more marked on moderately distending the stomach with air.
Percussion is also of use in ascertaining the presence of fluid in the peritoneum, whether from ascites or from extravasation; and, in the diagnosis of subphrenic abscess, by showing the extent to which the liver is depressed by the fluid above it, and by revealing a hyper-resonant note above the liver if the abscess contains air and fluid, this being changed to a note of dulness when the patient is rotated on to the affected side- Auscidtation, when combined with percussion, may reveal the splashing sounds in gastric dilatation, and the gurgling or metallic sounds in the cavity of a subphrenic abscess containing gas; the combined methods are also of use in mapping out the extent of gastric dilatation.
When the stethoscope is placed over the stomach, and percussion is made by tapping a coin placed on the abdominal wall by means of another coin, the area of gastric resonance may be readily mapped out.
In a healthy person food occupies about four seconds in passing from the mouth to the stomach, but where there is stricture of the oesophagus the time may be delayed for from fourteen to sixteen seconds ; this can be readily ascertained by auscultating- about three inches below the left scapula, at which point the gurgle or amphoric rushing sound can be heard when fluid enters the stomach. This may be important when the question of gastrostomy for cancer of the cardiac orifice or for stricture of the oesophagus arises.
Continue to:
- prev: Chapter III. General Diagnosis Of Stomach Diseases, Including Cancer
- Table of Contents
- next: Instrumental Aids To Diagnosis
Tags
stomach, operation, cancer, tumour, ulcer, gastric, gastrectomy