Case XXIV
Description
This section is from the book "Cancer And Other Tumours Of The Stomach", by Samuel Fenwick. Also available from Amazon: Cancer and other tumours of the stomach.
Case XXIV
A carpenter, aged fifty-six, was admitted into the London Temperance Hospital with the following history. He had always been in good health until five months previously, when he was suddenly seized with a bilious attack, and vomited for two days. Since that time he had suffered from flatulence and discomfort after meals, loss of appetite, and steady emaciation. Latterly he had vomited once or twice each day, and had become very weak. The bowels were confined, and micturition was accompanied by a scalding pain in the penis. On examination the patient was found to be very thin and anaemic, with a purple flush on either cheek, which was stated to have developed during the course of his illness. The pulse was small and compressible, the tongue covered with a creamy fur, the breath offensive, and the temperature sub-normal. The bowels were confined, but the stools contained bile. The lower border of the stomach extended nearly one inch below the level of the navel, and its pyloric portion appeared considerably dilated, since a succussion splash could be obtained as far outwards as the right anterior axillary line. The organ could be seen to contract slowly from left to right. The liver was enlarged, and the lower edge projected one inch below the costal margin (fig. 59). There was neither ascites nor jaundice, nor could any localised tenderness or tumour be detected in the abdomen. The thoracic viscera were normal. The vomit during the first night in the hospital amounted to eighteen ounces, and consisted of an alkaline opaque fluid of a deep green colour, which deposited a flocculent precipitate on standing. Gmelin's test gave a positive reaction, and after the addition of a few grains of bicarbonate of sodium the filtrate digested fibrin. The urine was much reduced in amount, and contained a trace of albumin. After the stomach had been washed out overnight, and no food taken in the interval, thirteen ounces of bilious fluid were extracted by a tube on the following morning, and even after the organ had been apparently emptied a splash could still be obtained to the right of the umbilicus. Daily lavage, combined with careful dieting, afforded considerable relief for the first ten days, but the loss of weight still continued. At the end of a fortnight it was noted that the patient was not so well. Vomiting occurred each night despite the lavage, and the right lobe of the liver had increased in size and presented a small superficial nodule. Attacks of extreme restlessness alternated with periods of somnolence, and at night-time he suffered from fits of choking, accompanied by urgent dyspnoea. On the eighteenth day after admission the bowels ceased to act and incessant vomiting set in, which lasted for three days and precluded the administration of nourishment by the mouth. During this period from six to nine pints of a thin alkaline green fluid were ejected every twenty-four hours. The urine was scanty, and assumed a dark red tint when boiled with nitric acid. A week later fluid was detected in the peritoneal cavity, and the patient complained of great distension after meals. A gland above the left clavicle was also found to be enlarged, and the nodule in the right lobe of the liver was more distinct. A few days afterwards the temperature suddenly rose to 101° F., and he became delirious. There was no cough or expectoration, and the respirations were only twenty-four per minute. The following day the temperature had fallen to 99°, but the patient was semi-unconscious, with a dry tongue and a pulse-rate of 136. Comparative dulness on percussion was detected at the base of the right lung, and a few moist crepitations were audible on auscultation. During the evening the temperature rose to 102°, the coma deepened, and death occurred in the early morning.
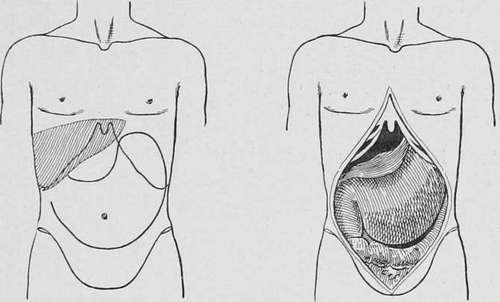
Fig. 59___Physical signs Fig. 60__Post-mortem appearances in Case XXIV. in Case XXIV.
Necropsy
The anterior portion of the abdominal cavity was chiefly occupied by two thin-walled sacs, which lay side by side. The one on the left consisted of a dilated stomach, while the other, which was ovoid in shape and eight inches in length, with a maximum circumference of thirteen inches, represented the upper two thirds of the duodenum in a state of extreme distension (fig. 60). When the latter was laid open, its lower end was found to be the seat of an ulcerated malignant growth, which had so contracted the lumen of the bowel that it hardly admitted the tip of the index finger. The retro-peritoneal glands were much enlarged, and the liver contained four secondary growths. There was recent pneumonia in the lower lobe of the right lung. The growth was a columnar-celled carcinoma.
Cases have been recorded in which the whole or greater part of the duodenum was infiltrated with carcinoma, and converted into a thick rigid tube of small diameter. The symptoms that accompany this rare form of disease are essentially those of chronic intestinal obstruction, accompanied by excessive vomiting and dilatation of the stomach. Jaundice is an inconstant phenomenon, but melaena is not infrequent. In Arrachard's case a large membranous cast was evacuated after the administration of an aperient, and death was preceded by troublesome diarrhoea.
Duration And Complications
In our series of cases the average duration of the complaint was about seven months, the extreme limits being three and eighteen months. As a rule the fatal event is due to exhaustion from inanition, but when it occurs at an early period it may take place from autointoxication or some other complication. Fatal haemorrhage has been recorded only twice, and perforation, with general peritonitis, is rare. An intra-peritoneal abscess is rather more common than in simple ulcer, and usually points at the umbilicus or makes its way towards the upper surface of the liver. Suppuration behind the peritoneum is very exceptional. Occasionally the growth produces an external fistula, or establishes a communication with the transverse colon or with the gall-bladder. In the case recorded by Trevelyan death occurred from tetany.
Continue to:
- prev: Carcinoma Below The Biliary Papilla (Cancer Of The Third Portion Of The Duodenum, Infra-Ampullary Or Juxta- Jejunal)
- Table of Contents
- next: Case XXIV. Continued