The Wrist And Hand. Surface Anatomy. Part 2
Description
This section is from the book "Surgical Anatomy", by John A. C. MacEwen. Also available from Amazon: Surgical Anatomy.
The Wrist And Hand. Surface Anatomy. Part 2
On the dorsal aspect of the hand the tendons can generally be easily made out, particularly when the fingers are hyperextended. The first dorsal interosseous muscle is chiefly responsible for the eminence which appears when the two first metacarpal bones are firmly approximated. The prominence of the knuckles at the metacarpo-phalangeal and interphalangeal joints is formed by the heads of the proximal bones, and, therefore, when seeking to open these joints when flexed, the knife should be entered distal to the prominence.
The skin over the back of the wrist and hand is firmer than that of the palm, and freely movable. It is provided with numerous hairs and sweat-glands, and permits of the superficial veins being seen through it. Boils and furuncles not infrequently appear on this surface in connection with the hair or glands, but do not occur on the palm.
The subcutaneous tissues are very lax, permitting great oedematous swelling and accumulations of blood or pus. The venous plexus forms a network on the backs of the fingers, which collects to form a venous arch on the back of the hand, with the convexity pointing downwards, and which leads to the radial vein on the outer side, while on the inner side it is joined by a vein from the little finger, which runs in the fourth intermetacarpal space (vena salvatella) to form the ulnar veins. All the larger veins of the hand are on the dorsal aspect, and most of the blood of the hand returns dorsally. The lymphatics are large, and widely distributed over the dorsum. The nails grow about 1/32, inch per week, and are frequently marked by transverse grooves in illness or from injury. They are also said to be altered in shape by some diseases, and they share in clubbing of the finger-tips, which occurs in certain chest affections, becoming markedly curved (Hippocratic hand). The matrix of the nail receives a large branch from each digital nerve, and is extremely sensitive to injury or inflammatory processes. Such inflammatory conditions affecting the matrix are referred to as onychia (or paronychia, when the surrounding parts are affected), and may lead to deformity or destruction of the nail, a new nail forming if the matrix survives.
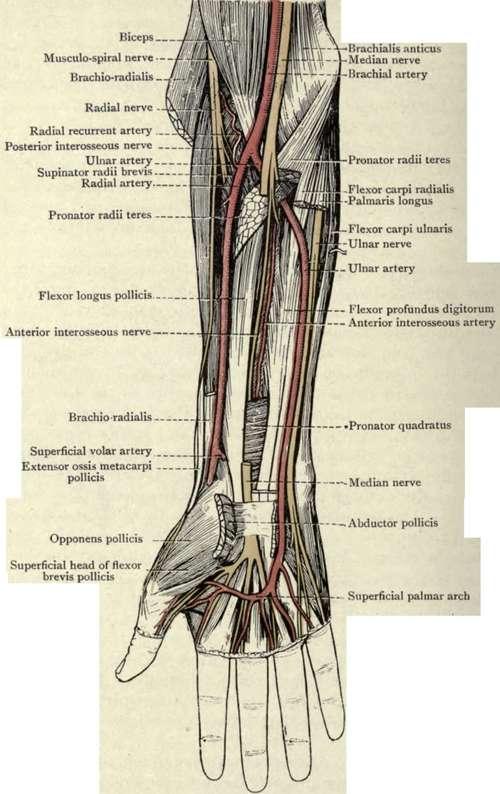
Fig. 56.-Deep Dissection of Front of Right Forearm, and Superficial Dissection of Palm. (From Buchanan's "Anatomy.')
The skin of the front of the wrist and hand varies much in character. On the front of the wrist it is thin and comparatively movable, but is connected with the deep fascia. The superficial veins are visible through it, and the median vein of the forearm generally takes origin about this position. The skin over the thenar eminence is also thin, much thicker over the hypothenar eminence, and very thick over the palm, where, in addition, it is firmly bound down to the palmar fascia by numerous fibrous septa. The cuticle is thick, and both on palm and fingers presents numerous fine ridges, on which open large numbers of sweat-glands (2,800 per square inch on the palm). The papillce of the fingers are richly supplied with Pacinian corpuscles, the sensation of touch being more active on the palmar aspect of the terminal phalanx of the index-finger than on any other part of the body, except the tip of the tongue. The dorsum, on the other hand, is much less sensitive, while the skin of the middle of the forearm and of the shoulders is very insensitive. There are no hairs, sebaceous glands, nor large superficial veins, and few lymphatics on the palmar aspect.
The subcutaneous tissue is dense and scanty, the fat being arranged in lobules between the fibrous septa. It is continuous with that of the forearm and fingers, and with the fatty tissue in the central compartment of the palm, between the slips of the palmar fascia. It is also continuous laterally with that on the dorsum. Over the proximal and middle phalanges it is connected with the fibrous sheaths of the flexor tendons, while on the distal extremity of the terminal phalanges it forms the pulp of the finger, which is intersected by numerous trabecular passing from the skin to the periosteum of the bone (cutaneous phalangeal ligaments of Cleland). These trabecular are of importance in suppurative affections of the terminal phalanges, as they tend to direct the process downwards from the surface to the periosteum, whereby .a simple whitlow may give rise to a subperiosteal abscess, or paronychia, with partial necrosis of the bone, the epiphyseal end, to which the flexor profundus is attached, generally surviving (the epiphysis unites about the twentieth year).
The palmar fascia is strong and unyielding, is comparatively free from vessels and nerves, and hence renders the overlying skin suitable for withstanding pressure and friction. The infunate connection between skin and fascia also prevents gaping of wounds and accumulations of oedema or blood ; indeed, when inflammation does occur in this region, it generally produces much pain from tension of the parts. The palmar fascia consists of a stout central palmar portion, and two lateral expansions to the thenar and hypothenar eminences, by which these latter are enclosed. The central portion is connected superficially with the skin by numerous septa, but its deep surface, lying over the flexor tendons, is smooth. Commencing above where it is continuous with the anterior annular ligament and palmaris longus muscle, it widens out as it approaches the fingers, and divides opposite the heads of the four inner metacarpal bones into four slips, which pass to the roots of the respective fingers. These again divide, and pass to the sheaths of the flexor tendons, transverse metacarpal ligaments, and skin. This fascia is so dense that suppurative processes can hardly come forward through it, but are generally forced down along the fingers, or up into the forearm, or even back on to the dorsum of the hand.
Continue to:
- prev: The Wrist And Hand. Surface Anatomy
- Table of Contents
- next: The Wrist And Hand. Surface Anatomy. Part 3