The Pyriformis
Description
This section is from the book "Surgical Anatomy", by John A. C. MacEwen. Also available from Amazon: Surgical Anatomy.
The Pyriformis
The glutei medius and minimus are also provided with bursae over the great trochanter, into which, along with the Pyriformis, obturator internus and gemelli, they are inserted. The bursa over the ischial tuberosity is frequently enlarged, giving rise to the condition known as Weaver's or Lighterman's bottom. It may cause pressure on the perineal branch of the small sciatic nerve, giving rise to unilateral neuralgia of the penis and scrotum. Pressure on the same nerve as it crosses in front of the tuber ischii from the use of a hard seat may give rise to similar neuralgia, temporary numbness, or anaesthesia. Small branches of the gluteal and sciatic arteries and nerves pierce the gluteus maximus, while under it lie two groups of vessels and nerves-those which emerge above and below the pyriformis muscle. Those which emerge aòove are the gluteal vessels (posterior division of the internal iliac) and superior gluteal nerve from the sacral plexus, which latter supplies the gluteus medius and minimus, and tensor fasciae femoris. The artery anastomoses with the deep circumflex iliac of the external iliac, the external circumflex of the profunda femoris, and the sciatic artery. It is generally about the size of the ulnar, but may be larger, and has caused death from haemorrhage when wounded. As a rule, however, the trunk escapes, as it is situated chiefly within the pelvis. The trunk is occasionally the seat of aneurism, which, pressing on the lumbo-sacral cord, gives rise to nerve symptoms. Below the pyriformis are the sciatic vessels and nerves, and the nerve to the quadratus femoris. In addition, the internal pudic vessels and nerve, and nerve to the obturator intern us, emerge from the great sciatic foramen, turn round the ischial spine, and re-enter the pelvis through the lesser sciatic foramen. The sciatic artery from the anterior division of the internal iliac supplies the surrounding muscles, anastomoses with the other vessels, and supplies a branch to the great sciatic nerve. The sciatic, internal and external circumflex, and the first perforating vessels form the crucial anastomosis about the level of the quadratus lumborum. Very rarely the femoral artery extends down the back of the thigh instead of the front.
The great sciatic nerve, the largest in the body, is a continuation of the sacral plexus (fourth lumbar to third sacral), and lies midway between the tuber ischii and the great trochanter. It is a frequent seat of neuralgia, called here sciatica, which may be due to pressure in the pelvis from tumours, engorged pelvic veins, aneurism of branches of the internal iliac, sciatic hernia, faecal masses in the rectum, etc., while below the gluteus maximus it is comparatively superficial, and may be exposed to cold or injury. It may be stretched by flexing the extended limb on the abdomen, or it may be cut down on, picked up at the lower margin of the gluteus maximus, and stretched by hand, the pelvis being raised by it from the table. A weight of 183 pounds is said to break the nerve.
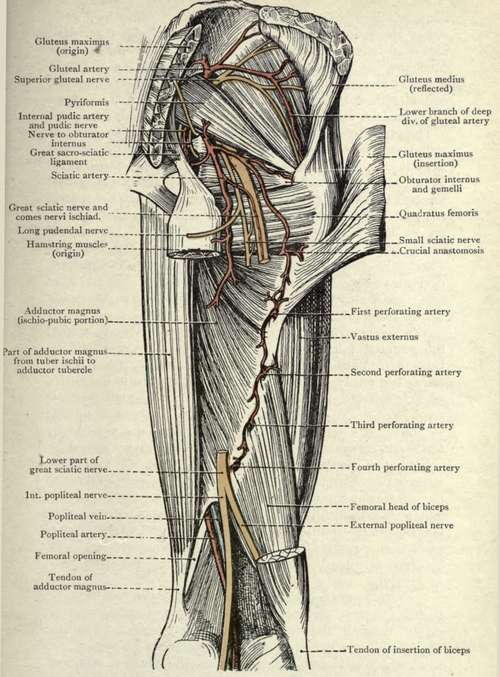
Fig. 35.-The Gluteal Region and Back of the Thigh. Deep Dissection. (From Buchanan's " Anatomy. ")
The gluteal region is richly supplied with nerves, and has well-developed tactile sensation. The nerve-supply is derived from the twelfth dorsal, first lumbar, second and third sacral segments (the latter segments also supplying the sexual organs) ; through the lateral cutaneous of the twelfth dorsal, twigs from the posterior branches of the lumbar and external cutaneous nerves, iliac branch of the ilio-hypogastric, and branches of the sacral nerves and of the small sciatic. The following muscles lie under the gluteus maximus : the gluteus medius, pyriformis, the obturator internus, with the gemelli on either side ; quadratus femoris ; hamstrings arising from the tuber ischii ; adductor magnus ; and vastus externus.
The great sacro-sciatic ligament stretches downwards from the posterior inferior iliac spine, sacrum, and coccyx to the tuber ischii, while the lesser sciatic ligament stretches downwards and outwards from the side of the sacrum to the ischial spine. The latter converts the great sciatic notch into the great sacro-sciatic foramen (which is bounded on its inner side by the great ligament), while the great ligament, assisted by the lesser, converts the lesser notch into the lesser foramen.
Wounds of the gluteal region, especially those entering behind the great trochanter, may readily penetrate the pelvis through the sciatic notch, and damage the bladder, ureter, or rectum, giving rise to fistulae, while the peritoneal cavity may be opened and peritonitis result. The gluteal and sciatic arteries have been ligatured from the gluteal region, and might be involved in wounds, while the great sciatic nerve might also be involved.
A sciatic hernia occasionally makes its way through the great sciatic foramen, and appears above the pyriformis muscle ; rarely through the lesser foramen, appearing below the pyriformis. Such herniae are more common in women, are generally small, and entirely under the gluteus maximus. When large, however, they may appear under its lower border.
The neck of the sac is usually situated at the fossa ovarica in the angle between the internal iliac artery and its obturator brancrr.
Treatment should consist in cutting down and out along the ilio-trochanteric line parallel to the fibres of the gluteus maximus, which are separated and retracted. The sac is then carefully defined and freed from adhesions, remembering that most of the vessels and nerves run down and outwards parallel to the fibres of the pyriformis.
Continue to:
- prev: Section IV. Lower Extremity. Gluteal Region. Surface Anatomy
- Table of Contents
- next: Scarpa's Triangle. Surface Anatomy