Operation Of Tying The Arteria Innominata
Description
This section is from the book "Anatomy Of The Arteries Of The Human Body", by John Hatch Power. Also available from Amazon: Anatomy of the Arteries of the Human Body, with the Descriptive Anatomy of the Heart.
Operation Of Tying The Arteria Innominata
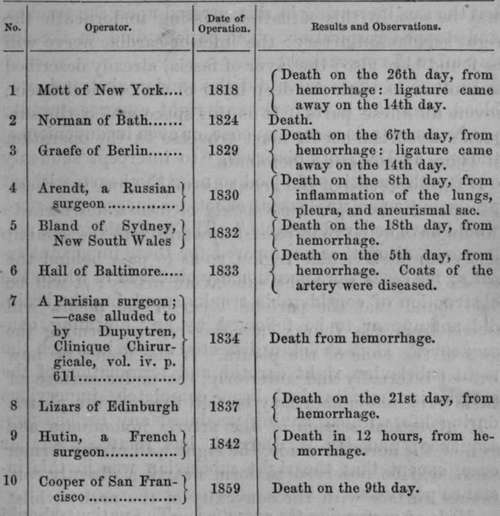
This operations has been performed in about ten cases: in nine for subclavian aneurisms; and in one, where hemorrhage took place after ligature of the subclavian: all these cases were attended with fatal results.
Ligature Of The Arteria Innominata
In the year 1831, Professor Porter, of this city, exposed the artery for the purpose of including it in a ligature, but, finding it diseased throughout its entire length, he thought it advisable not to tie the vessel: the wound was therefore closed. After some time the tumor had undergone considerable diminution in size, and when the patient left the hospital it had become nearly consolidated, and the pulsation had almost ceased.* A nearly similar case occurred in the practice of Mr. Key. The operator attempted to pass the ligature round the arteria innominata, but did not persevere. On the 18th day the patient was going on tolerably well, but the sac, increasing in size, pressed upon the trachea, and stopped respiration. The patient died on the 23d day after the operations.
In none of these cases did the sudden abstraction of blood from the head, neck, and right upper extremity produce any serious consequence, or even inconvenience; though, as Dr. Mott observes, "to intercept suddenly one-fourth quantity of blood so near the heart, without producing some unpleasant effect, no surgeon, a priori, would have believed possible." The profession were not, however, altogether unprepared for these important results; for cases were occasionally observed in which the obstruction of considerable trunks supplying the brain, did not appear to be followed by any alarming consequence. Thus Pelletan dissected a case in which the right subclavian, right carotid, and termination of the arteria innominata, had been completely impervious during life, without having produced any serious consequence; and Mr. W. Darrach has related a similar case, except that the right subclavian was in this instance pervious.
Mode Of Performing The Operation
The patient should lie on his back on a table, with both the shoulders thrown forwards, the right being at the same time drawn forcibly downwards, and the head leaning backwards, and to the left side. An incision should then be made transversely from the external margin of the sterno-cleido-mastoid muscle parallel to and above the clavicle, till it terminates opposite the trachea : a second incision is then to be made along the anterior margin of the sterno-cleido-mastoid muscle, about three inches in length, and terminating inferiorly at the internal extremity of the preceding incision. On raising the flap, the sterno-cleido-mastoid muscle is brought into view: under this a director should be conveyed from within outwards, keeping it close to the muscular fibres, in order to exclude the veins and nerves in this situation. On this we divide the sternal, and part (almost all, according to Guthrie) of the clavicular origin of the muscle. We then, by a similar proceeding, divide successively the sterno-hyoid and sterno-thyroid muscles of the right side above the sternum. With the nail, or handle of the scalpel, we should now tear through the dense aponeurosis covering the carotid artery, and in the same way dissect the small veins in this situation, not using the cutting edge of the knife as long as we can avoid it. When the carotid artery is exposed, it will serve (unless there be an irregularity) to conduct the finger to the arteria innominata, which, on account of the patient's position, will be drawn up from the thorax. The left vena innominata should now be depressed, and the aneurism-needle passed from without inwards and upwards, keeping it close to the vessel to avoid the pleura, and the pneumogastric and inferior cardiac nerves, all of which are on its right side. By tying the artery near its termination, there is more room left for the formation of an internal eoagulum. After the needle is passed underneath the vessel, considerable difficulty is often experienced in depressing its handle, so as to raise its point sufficiently on the opposite side: it became desirable, accordingly, that some means should be contrived to obviate this difficulty, and facilitate the conveyance of the ligature in deep situations. For this purpose a very ingenious instrument has been invented by Mr. L'Estrange, of this city.
* Dub. Jour. 1832, vol. i.
Crisp on " Diseases of the Blood-Vessels," p. 206.
Two other methods have been proposed to effect a ligature of the arteria innominata. The first is to trepan the upper piece of the sternum, and tie this vessel below the left vena innominata: this is a most objectionable proceeding. The second has been proposed originally by Dr. O'Donnell, of Liverpool,* and subsequently recommended by Velpeau: the following is an abridged account of it; the operator stands at the left side of the patient's head; an incision is to be made through the skin, commencing at the internal margin of the left sterno-mastoid muscle, and carried downwards and towards the right side for the extent of about two inches. The next incisions should divide the two layers of fascia in this situation, so as to expose the trachea. The middle thyroid artery, if present, and veins, are to be pushed aside, and, if necessary, tied. The index finger is now made to glide between the right sterno-hyoid muscle and the trachea, in order to detect the arteria innominata. The operator then passes a curved staff with great caution and management from before backwards, between the artery and vena cava superior. The posterior surface of the vessel is next to be denuded, and raised with the staff in the same cautious manner. Guided by this, the "stylet port fil" should be introduced from left to right, and from behind forwards. Velpeau says, that this operations is incontestably more simple, more rational, and less dangerous than any other; and has, moreover, this advantage, that the same proceeding will serve for the ligature of either of the sub-clavians in the first stage, or either of the carotids near its origin. Unfortunately, however, no matter how simple the steps of the operation may be made for including the arteria innominata in a ligature, the results of the operation have been so uniformly fatal that the surgeon has nothing to encourage him in its adoption.
* Cyclopaedia of Practical Surgery, vol. i. p. 260.
Continue to: