Roux's Operation. Part 3
Description
This section is from the book "Cancer Of The Stomach", by A. W. Mayo Robson, D.Sc, F.R.C.S.. Also available from Amazon: Cancer of the Stomach.
Roux's Operation. Part 3
There have been a number of cases recorded (14) in which closure of the artificial opening has occurred within a short time after the use of Laplace's forceps, and in others at a later time after the use of the Murphy button, and after the employment of Semi's plates.
Dr. W. J. Mayo (12) in a paper read before the American Surgical Association in June, 1902, reported four cases in which contraction at the site of anastomosis took place. These all followed the use of the Murphy button and occurred in cases where the pylorus was not occluded.
In operations for ulcer of the stomach it seems highly probable that the reason for want of relief in some of the cases has been owing to the anastomotic opening being made of too small a size, under which circumstances any subsequent slight contraction becomes of serious moment. This was demonstrated satisfactorily by Mr. H. J. Paterson in his Hunterian Lectures delivered at the College of Surgeons in 1906 (13).
(3) Peptic Ulcer Of The Jejunum
The subject of peptic ulcer is an extremely interesting one that has given rise to much speculation and to many theories.
In the stomach it is extremely common, in the duodenum probably much more frequent than hitherto supposed, but in the jejunum it is generally acknowledged to be very rarely found ; in fact it was only in 1899 that Braun first described the formation of peptic ulcer in the jejunum of man, and although the subject has since received attention in Germany by Hahn, Kausch, Korte, and others, my own case reported before the Royal Medical and Chirurgical Society on April 12th, 1904, was the first described in English literature. In that paper I referred to several cases, but I know that Mikulicz has since reported other cases, and several additional ones were collected by Mr. Paterson in his Hunterian Lectures.
As all of these cases were perforating ulcers, it almost goes without saying that there must be many more that have existed unrecognised, and probably others that may have caused death by abscess, and in other ways in which the adhesions and other complications have so obscured the parts that even an autopsy has failed to elucidate the true nature of the disease.
The true cause of peptic ulcer, whether gastric, duodenal, or jejunal, is probably a mild form of sepsis leading to gastritis and excess of free HCl in the gastric juice. Traumatism, either by coarse food or through external injury, and interference with the circulation in the bowel have been assigned as causes, but without what seems to me adequate reasons.
Peptic ulcer is distinctly one of the sequelae to be reckoned with after gastroenterostomy. An analysis of the cases shows it to occur more frequently after the anterior than the posterior operation.
As excess of free hydrochloric acid is not found in cancer of the stomach (except in ulcus carcino-matosum) it is hardly likely that peptic ulcer of the jejunum will be found after gastrojejunostomy for malignant disease, and so far as I know all the reported cases have occurred after operations for simple disease, especially ulcer. Nevertheless it is necessary to notice it here as one of the complications that may be met with.
As regards the frequency of peptic jejunal ulcers, out of nearly 300 posterior gastroenterostomies which I have personally performed I have not had one example.
My single case occurred after an anterior gastroenterostomy, 1 out of 30 that I have performed; and Kausch reported 2 out of 160 gastroenterostomies performed in Professor Mikulicz's clinic, both being after anterior gastroenterostomy.
Out of the 19 cases reported, the anterior operation had been done in 14, the posterior in 2, and the Y operation of Roux in 1 ; but whereas in the 2 cases of peptic ulcer occurring after the posterior operation, perforation was followed by general peritonitis, in the 14 anterior operations the peritonitis was limited in 9 and diffuse only in 5.
The symptoms in my case were evidently chiefly referable to the perigastritis and the extensive adhesions, and although there was intense and agonising pain at times, it seemed to bear no relation to food : exquisite tenderness over the upper abdomen was a marked feature of the case.
Treatment Of Peptic Jejunal Ulcer
In the cases of gastric ulcer that have failed to yield to medical treatment, and in which gastroenterostomy has been performed, I fear that we have not properly grasped the fact that the operation is, though an important one, still only an incident in the treatment, which ought to be continued on general lines for some time longer, or until good health is again established. Greater attention to oral asepsis and to the gastric condition of hyperchlorhydria subsequent to operation is advisable, and in this way the very serious complication of peptic ulcer in the jejunum and relapses in gastric ulcer might be prevented.
In all the cases reported, perforation associated with acute, subacute, or chronic symptoms, has occurred ; hence there can be no question as to the desirability-nay, as to the absolute necessity-of operation, which ought not to be delayed too long. When the abdomen is opened the treatment will depend on the condition found. If perforation has occurred into the general peritoneal cavity the condition will be one of the utmost peril, and only capable of relief by immediate cleansing of the peritoneum and closure of the opening, or by excision of the ulcer, with subsequent suture.
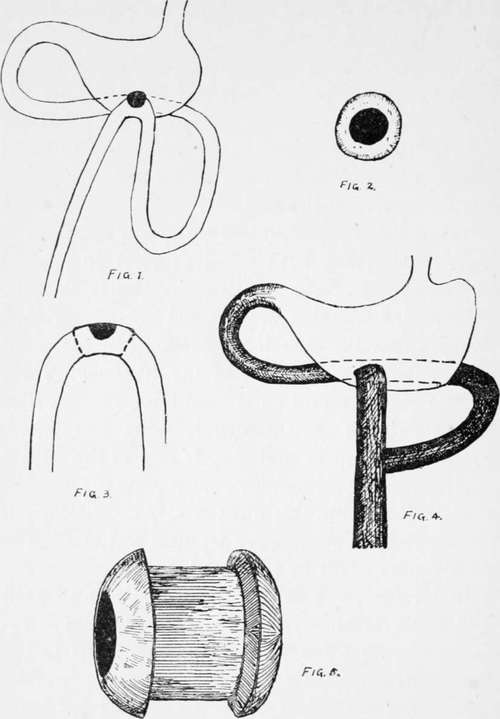
Fig. 20-1. Diagram of condition found on separating adhesions, May, 1903, showing perforation. 2. Diagram of portion of ulcer adherent to and detached from anterior abdominal wall. 3. Diagram of portion of intestine excised. 4. Diagram of anastomosis performed after the enterectomy. 5. Size of bobbins used. These five figures arc from page oil, vol. lxxxvii, Med.-Chir. Trans.
Continue to:
Tags
stomach, operation, cancer, tumour, ulcer, gastric, gastrectomy