Depage Method
Description
This section is from the book "Cancer Of The Stomach", by A. W. Mayo Robson, D.Sc, F.R.C.S.. Also available from Amazon: Cancer of the Stomach.
Depage Method
A. Depage (4) devised the following operation, which he successfully performed in a case of cancer of the upper part of the oesophagus when solid food could not be taken : A vertical incision 7 or 8 cm. long is made a little to the left of the middle line and at the seat of election. After opening the abdominal cavity, a portion of the stomach is drawn out and separated from the peritoneal cavity by a continuous suture which unites the wall of the organ to the edge of the peritoneum. A flap with its base upward is then cut out of the anterior wall of the stomach. This can be easily done by pinching up a piece of the wall between pressure forceps and cutting along the blades. The flap is then turned upward and the incision in the stomach is closed by a continuous suture, carried first only through the mucous coat. The serous layer is sutured in the same way. Each of the sutures is continued on to the flap, which is in this way transformed into a canal. The canal thus made is fixed to the abdominal wall, or if long enough it may be drawn through a parietal tunnel near to the xiphoid cartilage. The abdominal incision is then sutured and a sound is introduced into the canal, and may be left there or inserted before each meal.
This somewhat complicated operation is more difficult to perform, and at the same time is not more efficient than the other operations just described.
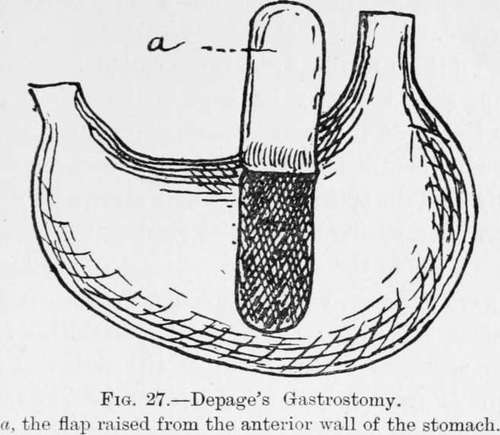
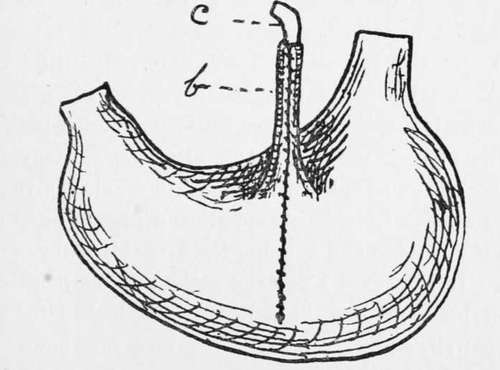
Fig. 28.-Depage's Gastrostomy.
The edges of the incision sutured together, and the flap transformed into a canal (6), through which a sound (c) is passed.
In all these methods a Jacques catheter, closed by a clip, should always be kept in the stomach for some length of time after operation, as the opening so readily contracts. In a recent case I have efficiently kept the opening patent by a short, solid, india-rubber plug, similar to the form employed for keeping open a sinus in the antrum.
I have performed my modified operation on many occasions and with most satisfactory results. Little or no shock is experienced, as although the peritoneum is opened there is neither exposure of viscera nor handling of any organ except the portion of stomach to be fixed, and I have never known peritonitis to follow.
Where the operation is not deferred until " too late," death should not occur except from some accidental complication : for instance, I lost a patient at the end of the first week after gastrostomy for cancer of the oesophagus from the unusual occurrence of an abscess caused by suppurating glands bursting into the trachea and flooding the bronchial tubes with pus. In that case I saw the patient in the morning, when he expressed himself as, and looked to be, doing well, and yet on returning in a few hours he was suffering from dyspnoea, was cyanosed and almost pulseless-in fact he died, drowned by pus, within six hours of the rupture.
Even after gastrostomy for malignant stricture of the oesophagus I have seen as much as 1^ st. to be gained in weight.
In one case in which I performed gastrostomy nearly seven years ago for what was supposed to be a malignant stricture, the patient gained his health and weight completely, and some time afterwards he regained the power of swallowing a little fluid, not sufficient, however, to support life, and he still makes use of his gastrostomy opening- for feeding purposes. He has a mere dimple to represent the site of the stomach fistula, into which he inserts without the slightest difficulty a No. 12 catheter a boule. There is no irritation around the opening, and even after so long a time there is no leakage of food or gastric fluid, so that he does not find it necessary to wear any apparatus or to have any dressing applied.
In advocating the earlier and more frequent performance of the operation of gastrostomy in cases of dysphagia incapable of relief by ordinary means, I feel that I can do so as the result of ample experience of its beneficial results.
References
1. Mayo Robson.-Practitioner, September, 1897.
2. Senn, E. J.-Journ. Amer. Med. Assoc., 1896.
3. Witzel- Cent.fur Chir., 1891.
4. Kader.-Cent, fiir Chir., 1896.
5. Depage.-Journ. de Chirurgie, December, 1901; Med. Reviev:, February, 1902.
Continue to:
Tags
stomach, operation, cancer, tumour, ulcer, gastric, gastrectomy