Tumors of Tongue
Description
This section is from the book "Skin Cancer", by Henry H. Hazen, A.B., M.D.. Also available from Amazon: Skin Cancer.
Tumors of Tongue
Like all other cancers of the skin and mucous membranes, carcinomata of the tongue do not arise de novo, but from some preexisting lesion. There is first an ulcer or a little area of infiltration that should give plenty of warning. These precancerous lesions may arise in various ways; they may be due to the irritation caused by bad teeth, or they may result from the excessive use of tobacco, either smoked or chewed. The latter must play some part, for cancer of this organ is very rare in women. Small papillary outgrowths of the tip or the lateral edges of the tongue are rather infrequent, but nevertheless do occur, and, even where there is no deep infiltration, they should always be removed, preferably with the electric cautery.
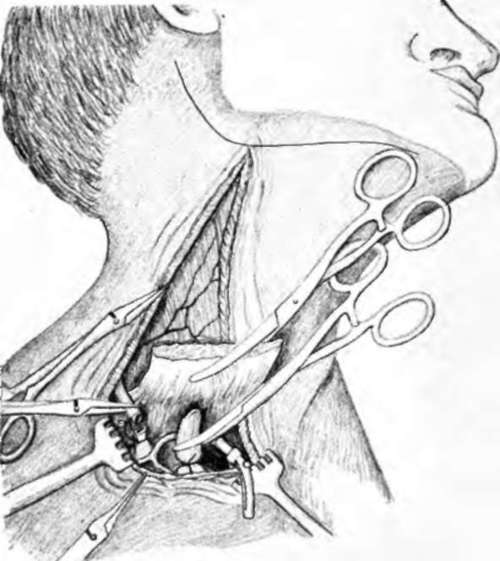
Fig. 94.-After the skin and subcutaneous tissue have been incised, the sternocleidomastoid muscle Is divided, the jugular veins ligated and cut, and the carotid artery is clamped. The skin and platysma are then dissected back. (Redrawn after Crile).
Syphilis is probably the most frequent cause of cancer of the tongue. Syphilis may produce either ulcers or superficial overgrowths, and these are very apt to undergo malignant change, especially in heavy smokers. The well-known leukoplakia, the so-called psoriasis or smoker's patch of the tongue, is often due to syphilis, although the use of tobacco must play a very important part. This ailment is characterized by the presence of superficial, white, slightly indurated patches, that have a tendency to form deep cracks and fissures. Many of them subsequently degenerate into true cancer. When leukoplakia is first seen, a thorough search for syphilis should always be instituted, and, if that is present, antisyphilitie medication should be pushed; in addition, smoking must be absolutely prohibited. If syphilis be not present, smoking should be forbidden and mild mouth wash prescribed. If the lesions yield promptly, as they sometimes do, operative treatment is not necessary, but, if the lesions still persist and especially if they increase in size, they should be thoroughly removed, preferably by either the actual or the electric cautery. In no case should they be touched with mild caustics or with any irritating substances; this is the worst thing that could possibly be done, for any form of irritation, short of complete removal, may stimulate cancerous changes.

Fig. 96.-The entire mass of lymph gland-bearing tissue is then excised en bloc. The dissection must be done in the deep plane of the neck. (Redrawn after Crile).
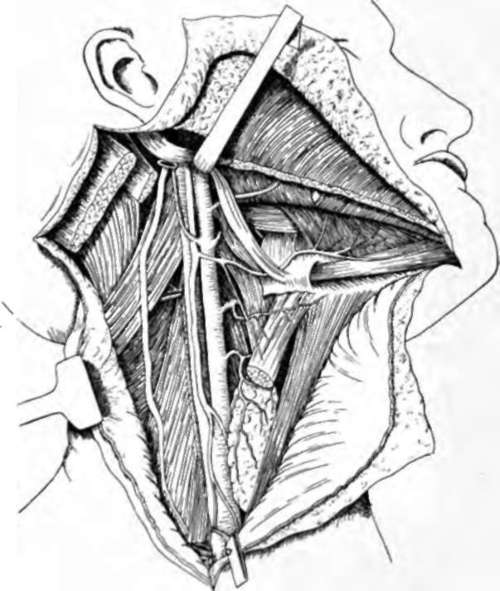
Fig. 96.-AH gland-bearing tissue has been removed, and the wound is ready to be closed. (Redrawn after Crile).
Tuberculous ulcers may likewise become cancerous, but, as a general rule, tuberculous lesions are rare, except in advanced tuberculosis of the lungs or in a generalized tuberculosis.
Any crack, fissure, or nodule should be viewed with suspicion until it is proven not to be cancerous. There are, of course, a number of lesions of the tongue that are perfectly benign; such a one is lichen planus, which often involves the mucous membranes of the cheek and which may invade the tongue. Occasionally we find a superficial infiltration of the surface, an infiltration that is sharply localized and rather angular, and that is most apt to occur in those who use either tobacco or snuff, and which seems to remain harmless. But in all cases of any abnormality a skilled man should be consulted.
Varieties
Various types of cancer may occur upon the tongue, but the common one is the spino-celled carcinoma, the type that speedily metastasizes. Cubo-celled growths also occur, but they are of mere pathological interest, for they are nearly as deadly as is the type just mentioned. The spino-celled wart also rarely occurs here; fortunately it does not metastasize, so local removal will suffice to give a cure. Basal-celled cancer, and rodent ulcers are extremely rare, and such a diagnosis should be received with the greatest caution. The pathology of all of these growths is identical with that of those already described.
Symptomatology
Cancer may develop upon any part of the tongue, but usually upon the dorsum near the edge, this being the part most exposed to trauma. Occasionally they develop primarily upon the floor of the mouth. As already indicated, there is always a precancerous lesion; it is noted that either deep induration or ulceration, or both, has taken place around this, and that an indurated ulcer, rarely a fungous tumor, results. Glandular involvement may occur within one month, and is rarely postponed more than six months. The floor of the mouth is often infiltrated at a very early date, nearly always within six months.
Diagnosis
The first difficulty is to determine whether a precancerous lesion has actually taken on a cancerous change, and how long this change has existed; this is always extremely difficult, for it is much easier to diagnose a late cancer than it is an early cancer, the only trouble being that, when a carcinoma is easily diagnosed, it is not easily cured. Hence there is only one safe rule, and that is to treat all such lesions as early cancers, and to have live patients at the end of a few years. In certain instances it is almost impossible to distinguish a gummatous lesion from a cancer. When one remembers that cancer so frequently develops upon a syphilitic basis, it can be readily seen that the Wasscrmaun reaction is more apt to prove a hindrance rather than an aid. In case of doubt, and if the lesion is advanced, it is well to give two or more intravenous injections of salvarsan at close intervals and watch the result. In the case of a small lesion the same procedure may be tried, or the whole lesion may be excised with the cautery and then studied microscopically. Tuberculous lesions may also be difficult to distinguish. In the case of very advanced tuberculosis it makes very little difference what the lesion is, but in other cases the differential diagnosis may be a matter of extreme importance. The whole lesion should be excised with the cautery, and the central portion studied microscopically and a bit of the fresh tissue injected into a guinea pig. This last is important, because tuberculosis may histologically resemble carcinoma.
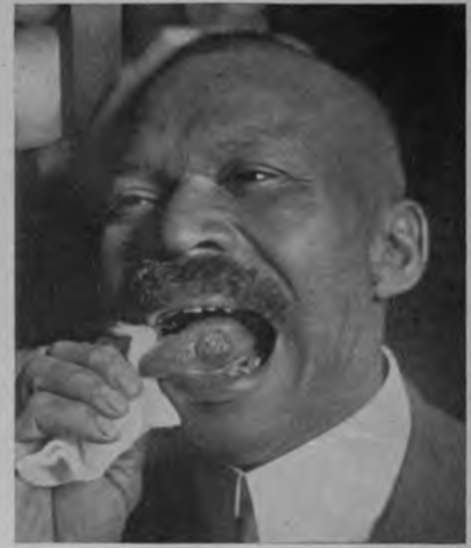
Fig. 97.-This cancer of the tongue Is of four months' duration. It had been treated with various caustics, which had apparently hastened its growth. (Photograph by Dr. Walter Van Swerirgen of Dr. H. H. Kerr's patient).
Continue to:
Tags
bookdome.com, books, online, free, old, antique, new, read, browse, download