Abdominal Tumour
Description
This section is from the book "Cancer And Other Tumours Of The Stomach", by Samuel Fenwick. Also available from Amazon: Cancer and other tumours of the stomach.
Abdominal Tumour
Tumours of the stomach vary so much in character, according to their situation, that in order to interpret their clinical significance aright it is necessary to bear in mind certain facts in connection with the position and relations of the normal stomach.
The adult stomach is situated in the left hypochondrium and epigastrium, with its long axis directed downwards and to the right. The median line of the body intersects the pyloric region in such a manner that nearly five-sixths of the organ lie in the left half of the abdomen (Luschka). The cardiac orifice is situated behind the seventh left costal cartilage, at its junction with the sternum, and is covered by the left lobe of the liver. The highest part of the viscus is the upper margin of the fundus, which reaches to the level of the fifth rib. The lesser curvature descends perpendicularly alcng the left side of the spinal column to the first lumbar vertebra, where it crosses abruptly to the right to terminate at the pylorus. When the stomach is empty the pylorus corresponds to the inner end of the eighth right cartilage just outside the parasternal line ; hut when the viscus is distended it may move two or three inches to the right of a line drawn from the tip of the ensiform cartilage to the umbilicus, while at the same time the great curvature comes nearer to the abdominal wall and the anterior surface looks more upwards. The lower border of the organ is very variable in its position, even in persons who enjoy perfect health, but as a rule it reaches as far as a line drawn between the cartilages of the ninth ribs.
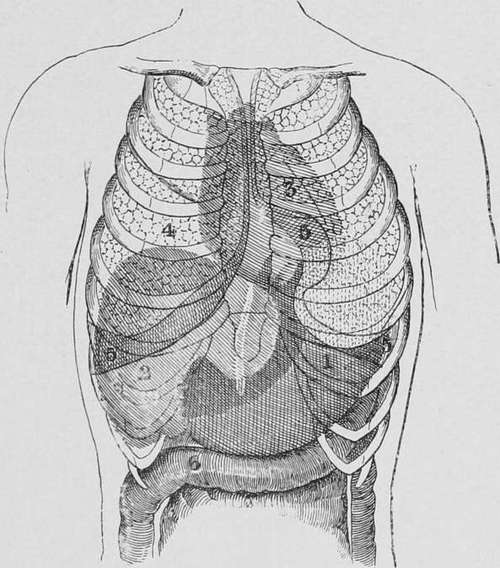
Fig. 39.-Situation of the normal stomach. 1, stomach ; 2, liver; 3, heart; 4, lungs ; 6, transverse colon. (Eichhorst.).
These facts indicate that only the lower halves of the pyloric and central thirds of the stomach come into contact with the anterior abdominal wall, and that, consequently, only those growths which are situated in these regions are invariably palpable. On the other hand, tumours of the cardia, of the fundus, or of the posterior gastric wall, are rarely felt until they have attained a considerable size or have occasioned dislocation of the stomach ; while those of the pylorus, by developing adhesions to the under surface of the liver, are also apt to escape detection.
Continue to:
- prev: Metastases In The Abdominal Wall
- Table of Contents
- next: General Characters Of The Gastric Tumour